Sleep Architecture: The Complete Science of Optimising Your Sleep Cycles for Peak Recovery and Cognitive Performance
Your body doesn’t need more sleep — it needs better-engineered sleep. The difference between waking sharp and waking foggy isn’t duration — it’s architecture.
The two-process model — mapped in the diagram alongside — — mapped in the diagram below — shows exactly how sleep pressure and circadian rhythm interact to control every aspect of your recovery.
Two forces control when you sleep — pressure builds, rhythm cycles.
Sleep architecture is how your brain organises each night into repeating cycles of light, deep, and REM sleep. Two internal systems control this — a pressure system that builds the longer you’re awake, and a clock system that tracks the time of day. When they’re aligned you sleep deeply and wake sharp. When they’re misaligned, no amount of time in bed compensates.
The Two-Process Model
Two independent forces control every second of your sleep — adenosine pressure and the circadian clock. Until you understand both, every sleep hack is a shot in the dark.
Sleep Stage Engineering
Deep sleep rebuilds your body. REM rebuilds your mind. But they compete for time within each 90-minute cycle — and most people are losing the wrong one.
Circadian Anchoring
Your suprachiasmatic nucleus runs a 24.2-hour clock that drifts without anchors. Light exposure, core body temperature, and meal timing are the three levers that lock it to solar time.
The Sleep Stack
Magnesium threonate, glycine, and L-theanine aren’t sedatives — they’re neurochemical precursors. This module builds the exact supplement, environment, and wind-down protocol for your chronotype.
Tracking & Iteration
Population averages are noise. Your HRV, resting heart rate, and sleep stage ratios tell a personal story. This module teaches you to read that data and iterate toward your biological optimum.
TLDR: 10 Sleep Tactics. 10 Recovery Myths Busted.
Everything below distilled into 20 cards. Deploy the tactics, debunk the myths. The full science follows after.
Why Sleep Optimization Is Non-Negotiable
You already know sleep matters. Everyone does. But here’s what most people don’t understand: sleep isn’t just recovery time—it’s the foundation upon which all other performance is built.
Time In Bed ≠ Sleep Quality
You can spend 9 hours in bed and wake up exhausted because your sleep architecture—the sequence and distribution of sleep stages—is degraded. Or you can spend 7 hours with optimized architecture and wake at 95% cognitive capacity.
This is why some people “function fine” on 5-6 hours while others feel destroyed after 7. It’s not just duration—it’s the quality of the cycles.
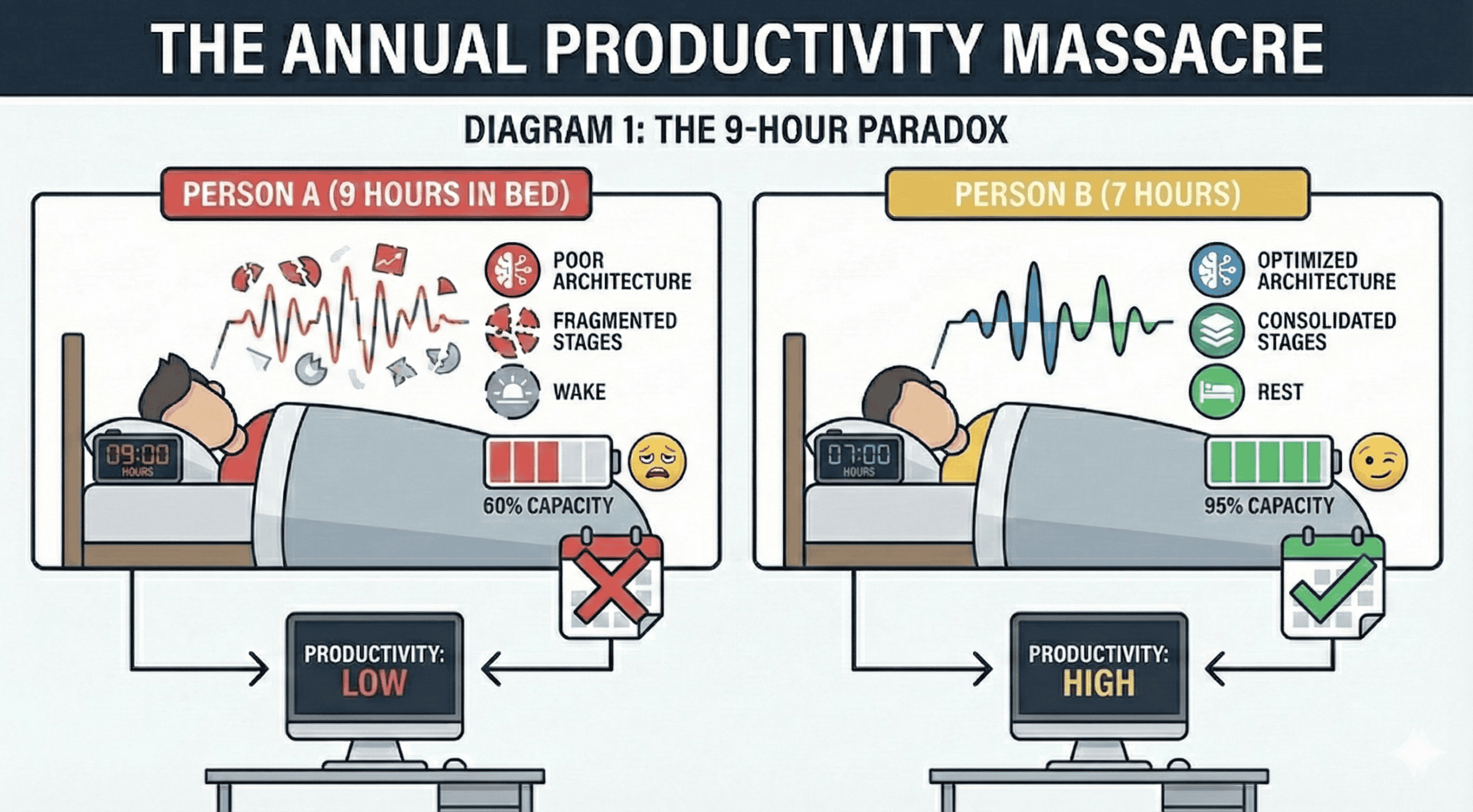
Annual Productivity Massacre
The Adaptation Trap
Here’s what makes this insidious: you don’t feel impaired. Studies show people chronically restricted to 6 hours report stabilized sleepiness ratings after 3 days—but their objective cognitive performance continues to decline linearly. You think you’ve adapted. You haven’t.
Sleep As Infrastructure
Stop thinking about sleep as a lifestyle choice. It is biological infrastructure. You cannot hack around these processes.
Deep Sleep (N3)
- Growth hormone release (80% of daily total)
- Physical repair & recovery
- Immune system strengthening
- Glymphatic activation (Brain waste clearance)
REM Sleep
- Memory consolidation (Procedural/Emotional)
- Synaptic pruning (Neural efficiency)
- Creative integration
- Emotional regulation
Light Sleep
- Sleep spindle activity
- Sensory processing integration
- Preparation for deeper stages
- Memory consolidation support
The Optimization ROI
What “Optimized” Looks Like
Most people are sitting on enormous performance gains they don’t even know exist. This isn’t theoretical—this is the documented experience of elite performers.
The Neuroscience of Sleep Architecture
What Is Sleep? (Quick Answer)
Sleep is a complex, multi-stage neurobiological process during which the brain systematically consolidates memories, clears metabolic waste, regulates hormones, and restores cognitive and physical capacity. It progresses through distinct stages (N1, N2, N3, REM) in ~90-minute cycles, with each stage serving specific restorative functions critical for performance.
What Is Sleep Architecture?
When scientists study sleep in a laboratory using polysomnography (the gold standard sleep measurement), they don’t see a uniform state. They observe a highly structured sequence of distinct brain states, repeating in cycles throughout the night. This structured progression—the pattern, timing, duration, and quality of each sleep stage—is what we call sleep architecture.
Understanding architecture is critical because all sleep is not created equal. The sleep you get from hour 1-2 (deep sleep dominant) serves completely different functions than hour 6-7 (REM dominant). Disrupt the architecture, and you disrupt the restoration—even if total duration remains the same.
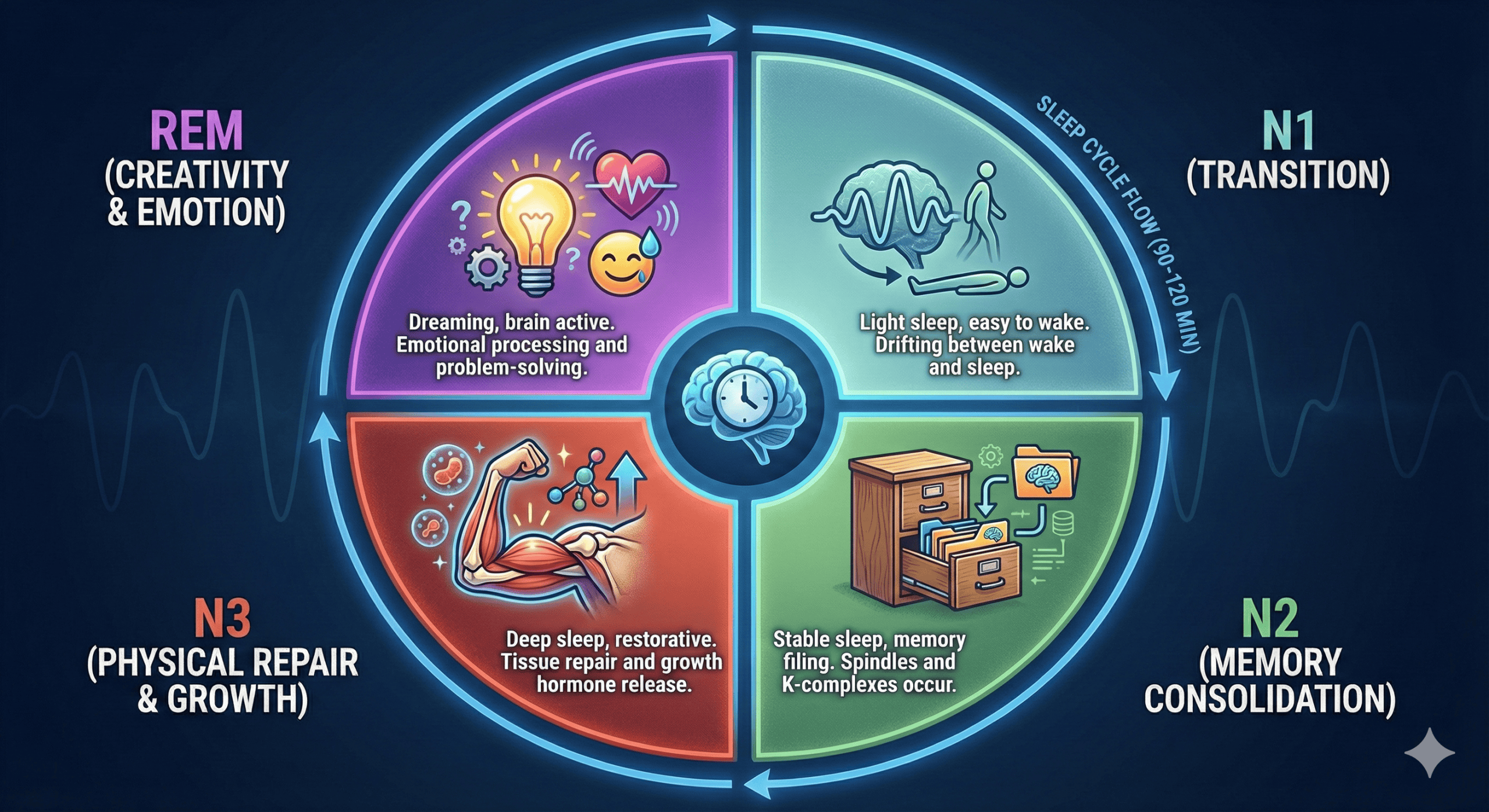 Fig 1.1: The Cycle
Fig 1.1: The Cycle
The Four Stages of Sleep
Sleep progresses through four distinct stages, classified by characteristic brain wave patterns, eye movements, and muscle tone:
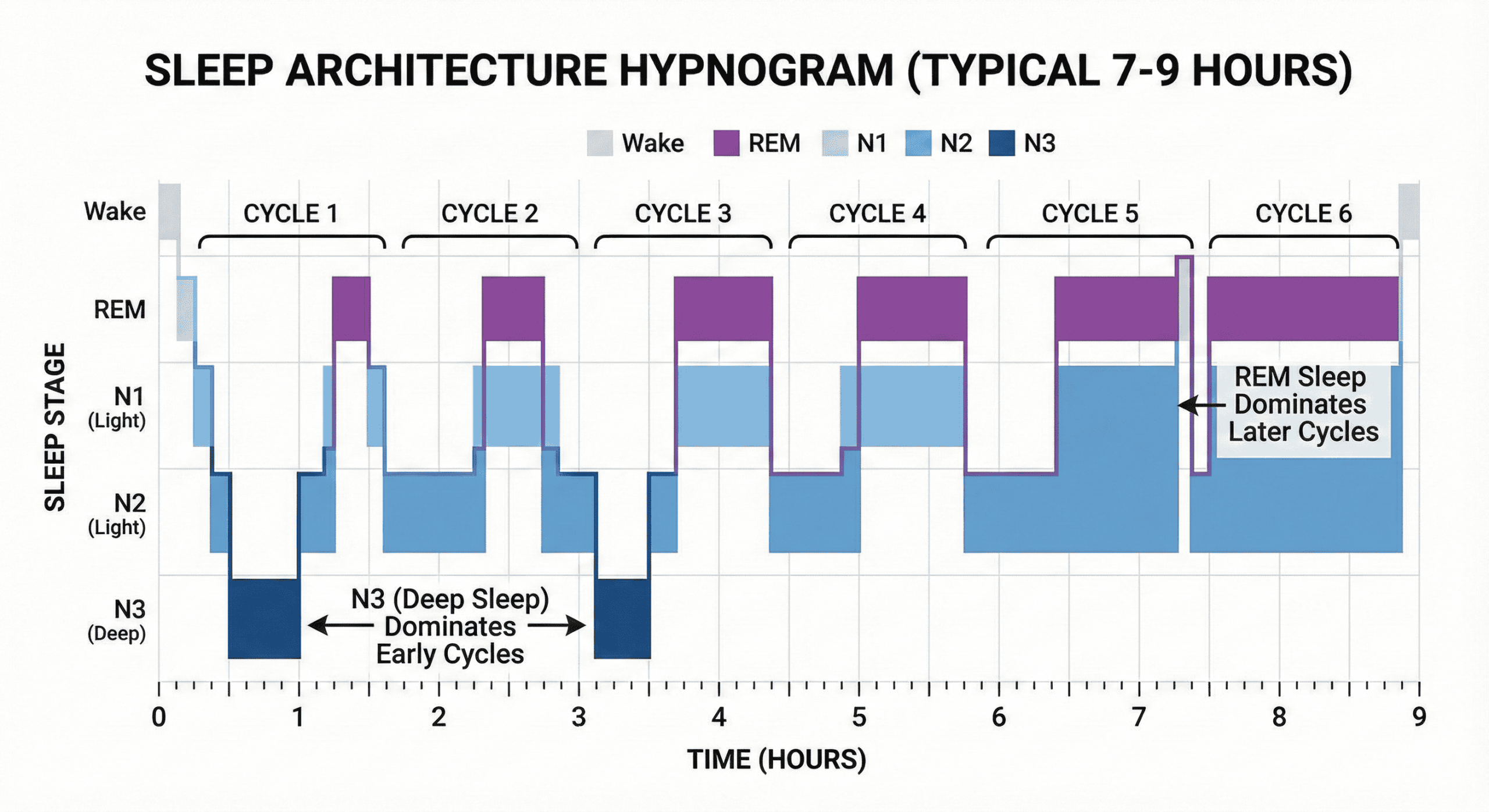 Fig 1.2: The Hypnogram
Fig 1.2: The Hypnogram
Sleep Cycles: The 90-Minute Pattern
Sleep doesn’t move linearly. It cycles in roughly 90-120 minute periods, repeated 4-6 times per night. Critical insight: Cycle composition changes dramatically across the night.
- Early Cycles (1-2): Deep sleep dominates (Physical Repair).
- Late Cycles (4-6): REM sleep dominates (Cognitive/Emotional Repair).
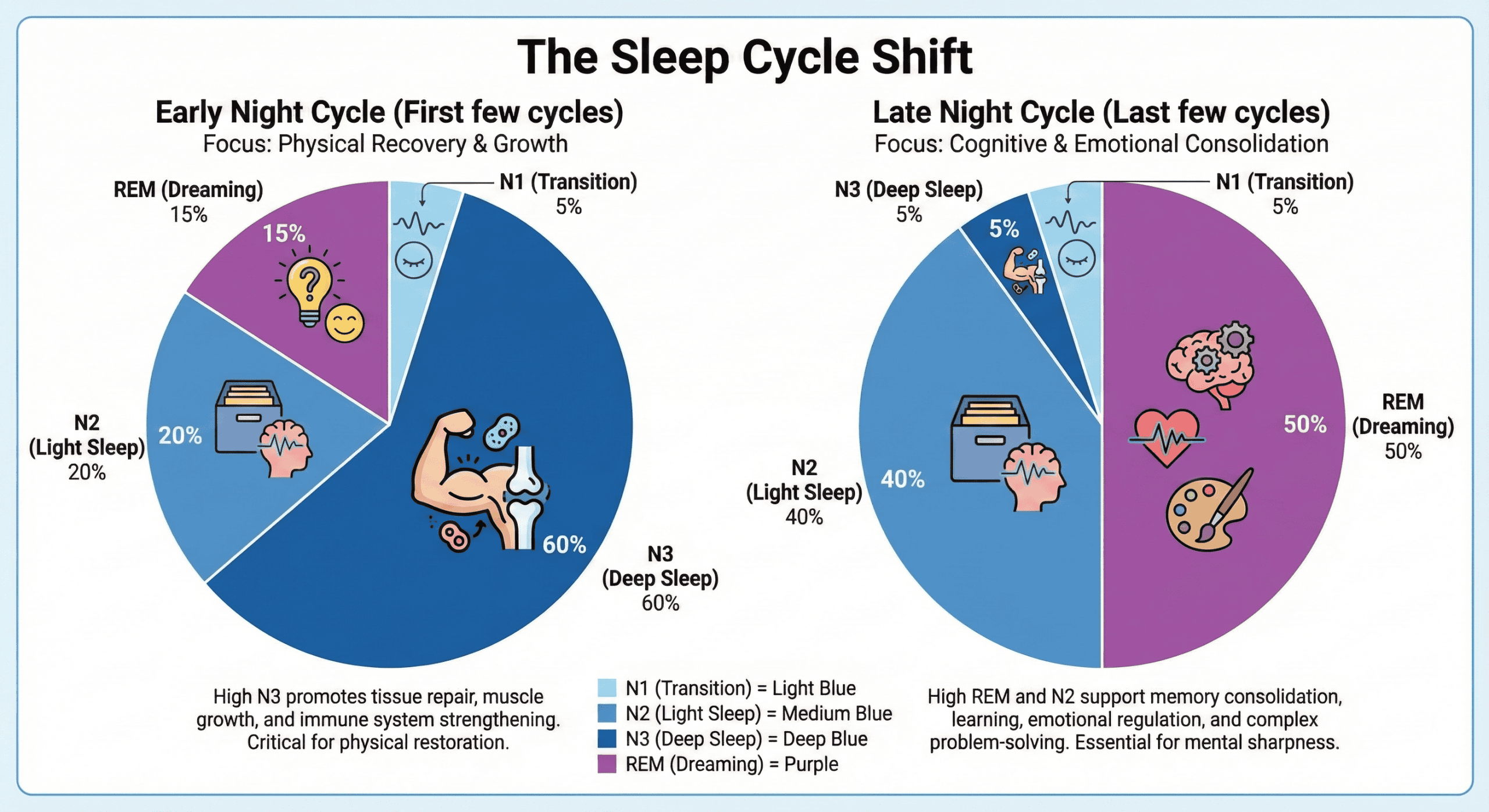 Fig 1.3: Cycle Composition
Fig 1.3: Cycle Composition
This distribution has profound implications. If you only sleep 6 hours (cutting the final 2 hours), you disproportionately eliminate REM-rich cycles—impairing memory consolidation and emotional regulation while maintaining some physical recovery.
The Two-Process Model
Why do you get sleepy at night? Two independent but interacting processes regulate your sleep-wake cycle.
Process S: Pressure
(Homeostatic Drive)
A rising tide of sleepiness driven by Adenosine accumulation. The longer you are awake, the higher the pressure.
Hack: Caffeine blocks adenosine receptors, masking this pressure without clearing it.
Process C: Rhythm
(Circadian Clock)
A 24-hour rhythm generated by the SCN (Suprachiasmatic Nucleus). It orchestrates temperature, cortisol, and melatonin.
Hack: Light is the primary “Zeitgeber” (time-giver) that anchors this rhythm.
Fig 1.4: Process S & C Interaction
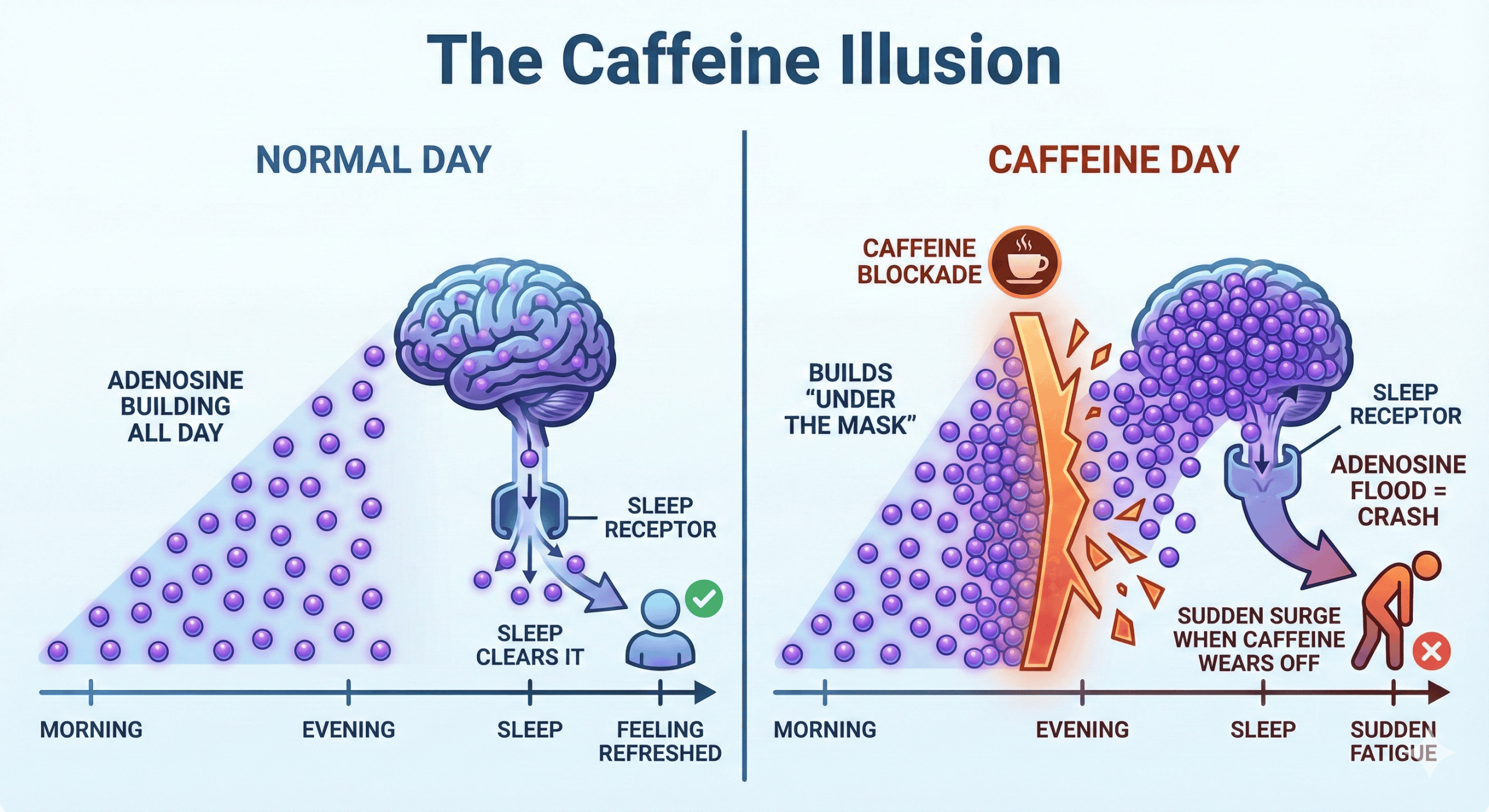 Fig 1.5: The Caffeine Illusion
Fig 1.5: The Caffeine Illusion
The Glymphatic System: Brain Waste Clearance
One of the most important discoveries in sleep neuroscience (2013). During Deep Sleep (N3), brain cells physically shrink by ~60%, allowing Cerebrospinal fluid (CSF) to flood the interstitial spaces.
This process flushes out metabolic waste, including beta-amyloid and tau proteins (associated with Alzheimer’s). If you aren’t getting deep sleep, you aren’t “taking out the trash.”
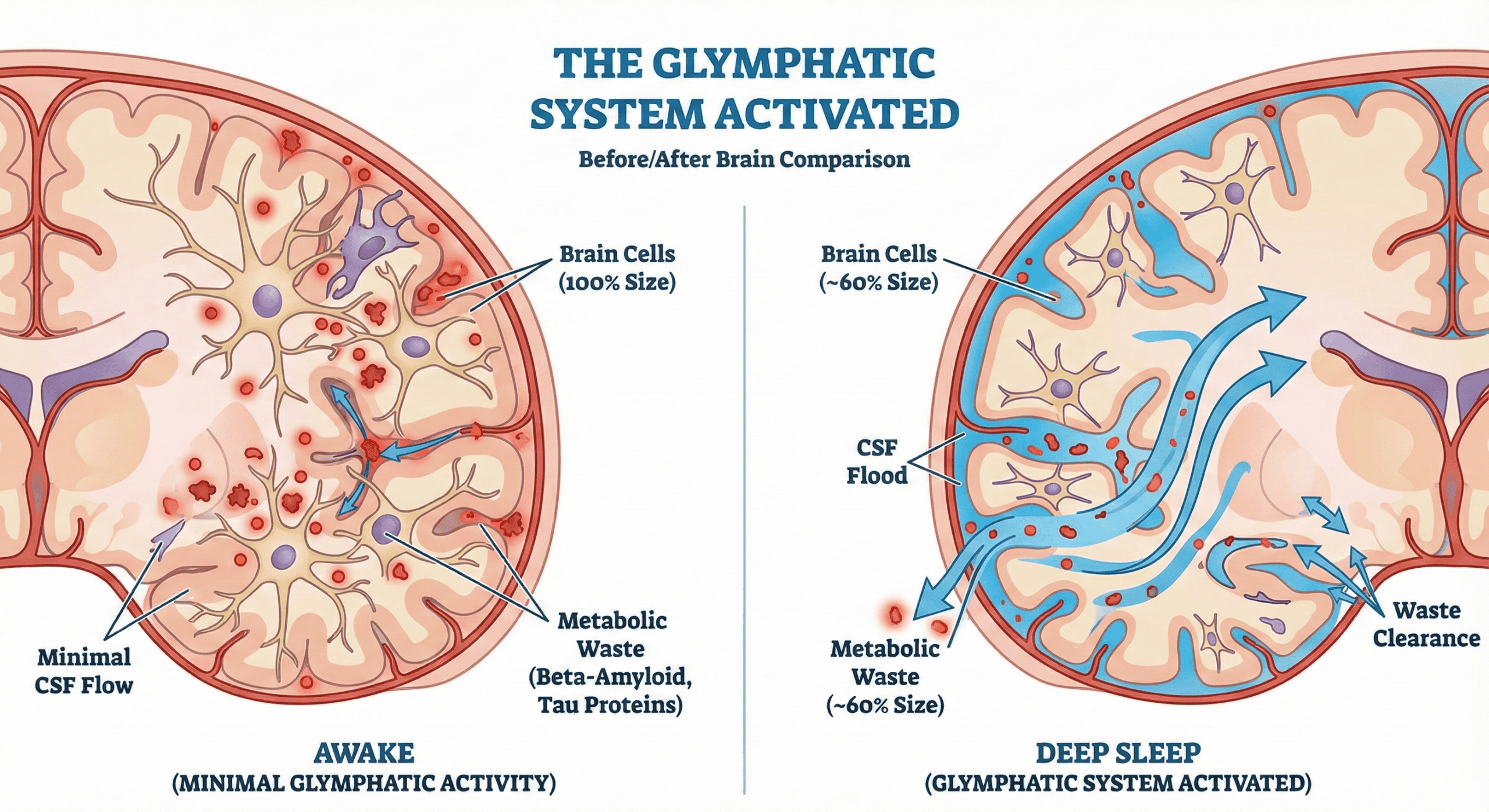 Fig 1.6: Glymphatic Activation
Fig 1.6: Glymphatic Activation
Memory Consolidation
Information is initially stored in the hippocampus (temporary RAM). During sleep, especially N2 Spindles and REM, this data is transferred to the neocortex (Hard Drive) for long-term storage.
- N2/N3: Fact-based (declarative) memory replay.
- REM: Skill-based (procedural) memory and emotional processing.
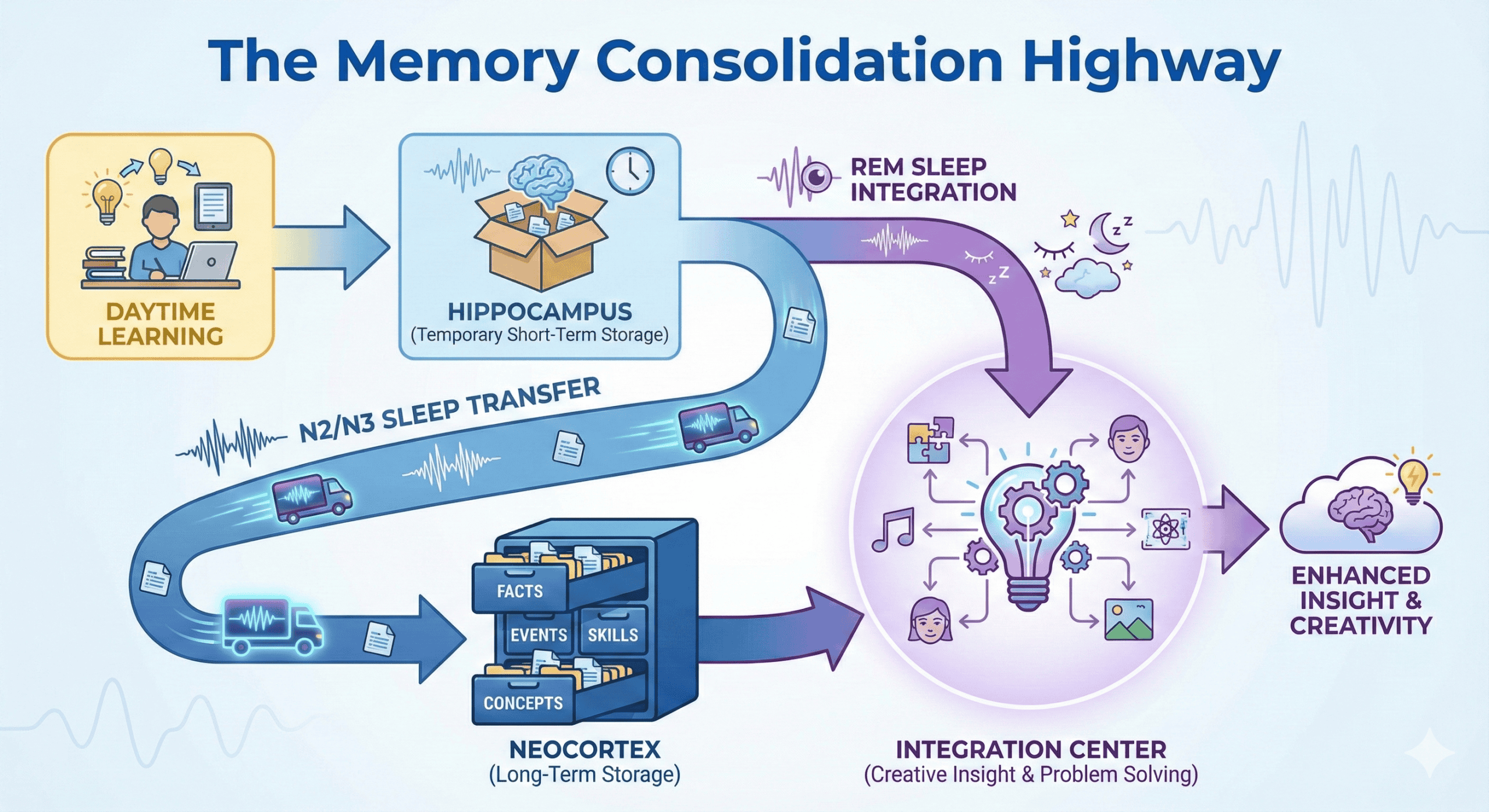 Fig 1.7: Memory Transfer
Fig 1.7: Memory Transfer
Summary: Sleep Stages & Performance
| Stage | % of Night | Primary Function | Degraded By |
|---|---|---|---|
| N1 | 5% | Sensory disengagement | Stress, Anxiety |
| N2 | 45-55% | Memory Consolidation (Spindles) | Alcohol, Frequent Arousals |
| N3 (Deep) | 15-25% | Physical Repair, Glymphatic Clearance | Age, Caffeine, Heat |
| REM | 20-25% | Emotional Regulation, Creativity | Alcohol, Early Waking, Cannabis |
The Four-Pillar Optimization Framework
Sleep architecture doesn’t optimize by accident. It requires systematic engineering across four interconnected domains.
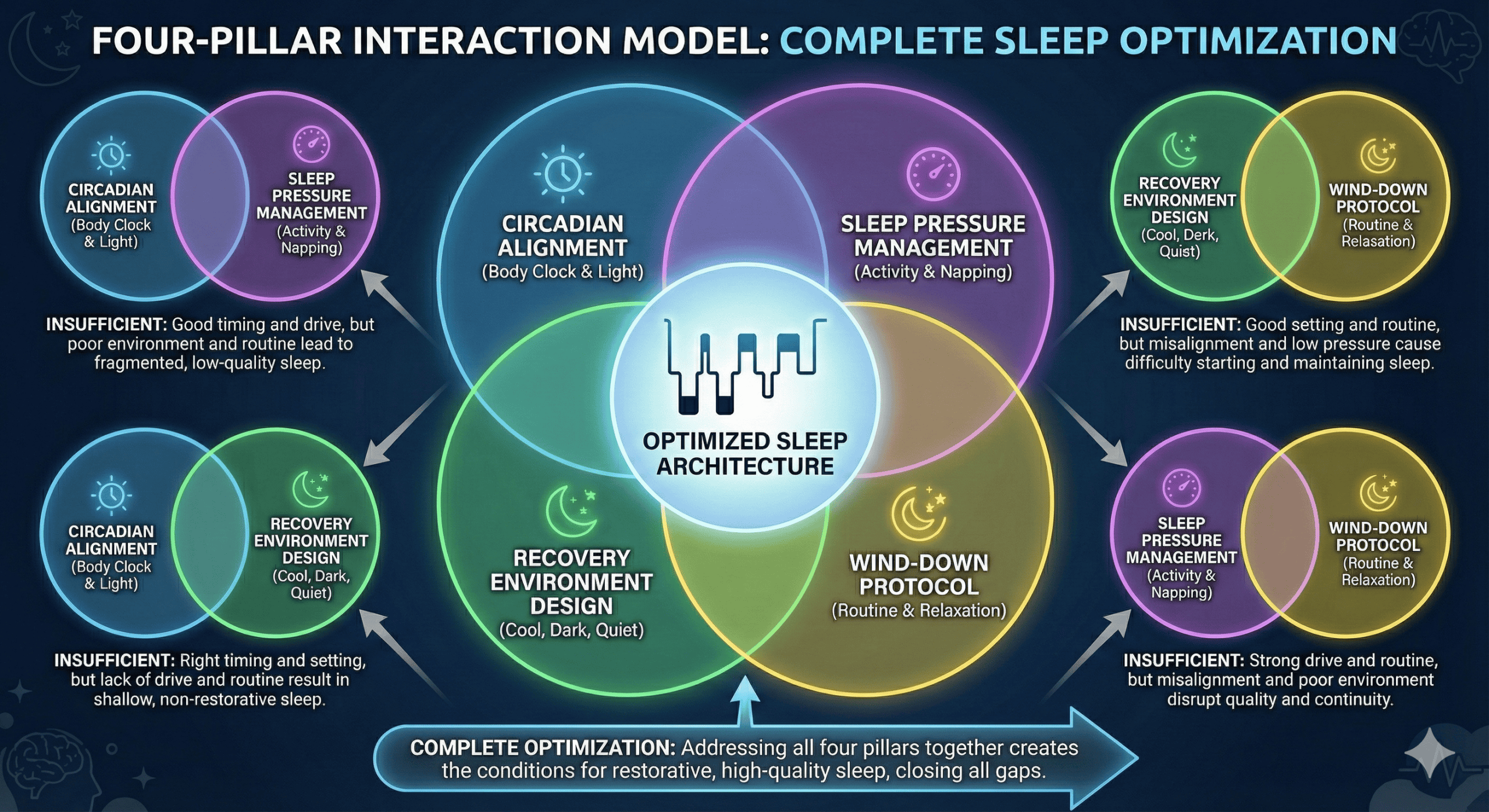 Fig 2.1: System Model
Fig 2.1: System Model
Each pillar addresses a different mechanism:
- Pillar 1: Circadian Alignment → Process C (your internal clock)
- Pillar 2: Sleep Pressure Management → Process S (homeostatic drive)
- Pillar 3: Recovery Environment Design → Sensory and physiological conditions
- Pillar 4: Pre-Sleep Wind-Down Protocol → Nervous system transition
Mastering all four creates compounding effects. Optimizing just one produces limited benefit. Optimizing all four synergistically creates dramatic sleep architecture improvement.
Circadian Alignment
Goal: Synchronize your sleep-wake cycle with your biological clock to maximize sleep quality and daytime performance.
Your circadian rhythm is a roughly 24-hour cycle generated by the suprachiasmatic nucleus (SCN) in your brain. This master pacemaker orchestrates sleep timing, hormone release, body temperature, and cognitive performance across the day.
The critical insight: Your circadian rhythm “wants” to run slightly longer than 24 hours (typically 24.1-24.3 hours). Without external cues, it would drift later each day. Light exposure is the primary “time cue” (Zeitgeber) that resets the clock daily and keeps it aligned with the 24-hour day.
The Light-Dark Cycle: Your Primary Circadian Tool
1. Morning light exposure: The Reset Signal
The single most powerful circadian intervention. It suppresses residual melatonin, triggers cortisol rise, resets circadian clock to “daytime mode”, and advances sleep phase (makes you sleepy earlier in evening).
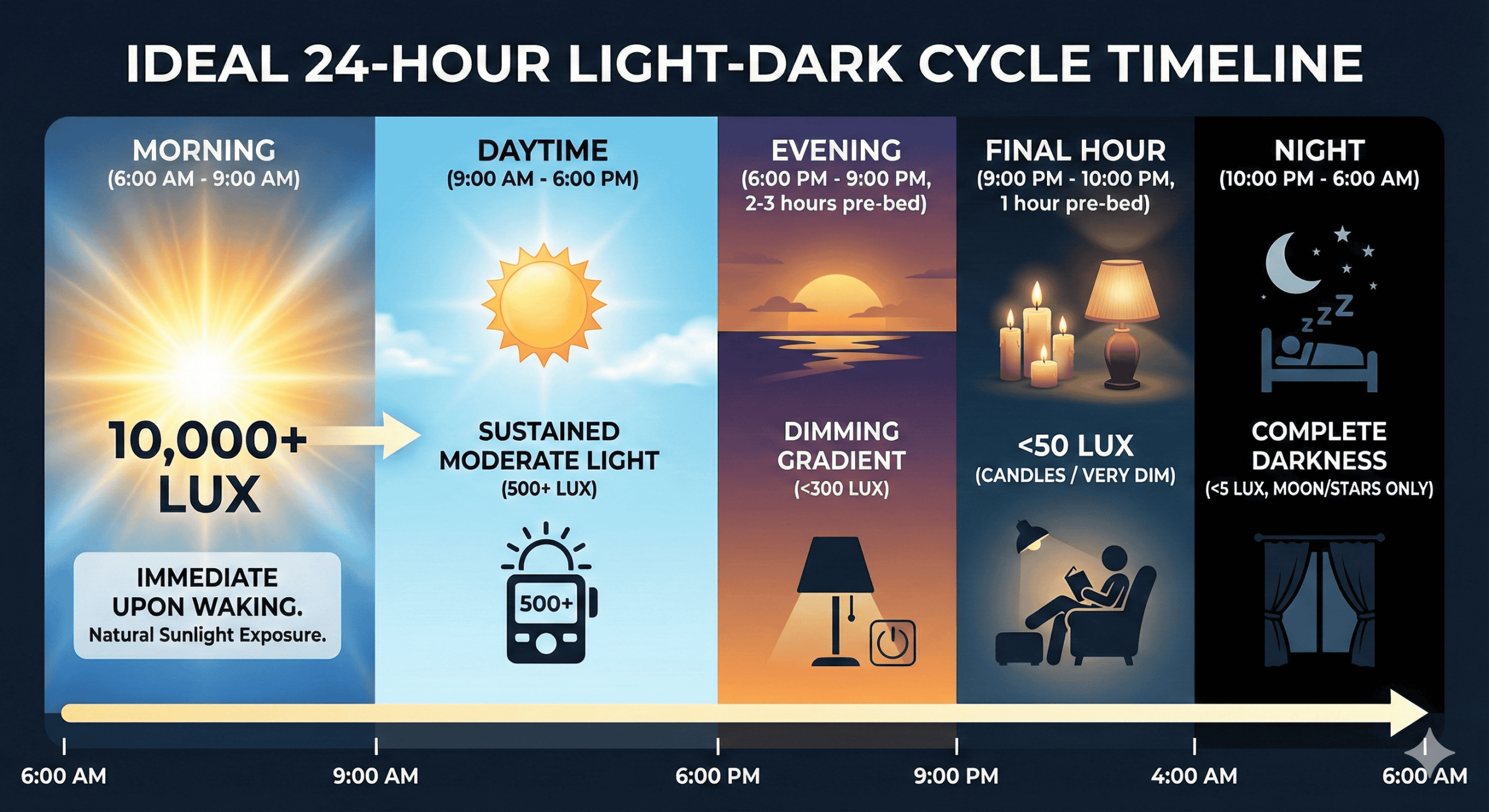 Fig 2.2: Ideal Light Timeline
Fig 2.2: Ideal Light Timeline
2. Evening light restriction: The Protection Signal
Allows melatonin to rise naturally, prevents circadian phase delay, and facilitates parasympathetic nervous system activation.
| Light Source | Typical Lux | Circadian Impact | Recommended Use |
|---|---|---|---|
| Direct sunlight | 50,000-100,000 | Strong phase advance, melatonin suppression | Morning exposure (10-30 min) |
| Overcast sky | 10,000-20,000 | Moderate-strong phase advance | Morning exposure acceptable |
| Office lighting | 300-500 | Mild circadian activation | Daytime work |
| Sunset | 400-1000 | Minimal (natural evening cue) | Evening transition |
| Typical living room | 100-300 | Mild melatonin suppression | Evening (acceptable if <300 lux) |
| Tablet/phone (bright) | 30-50 (at eye) | Moderate melatonin suppression | Avoid 2 hours before bed |
| Candles/dim lamps | < 50 | Minimal suppression | Ideal evening lighting |
| Darkness (sleep) | <1 | None (allows melatonin peak) | Sleep environment |
Consistent Wake Time: The Circadian Anchor
The principle: Your wake time is more important for circadian stability than your bedtime.
The SCN uses morning light exposure + consistent wake time as primary cues to set the clock. Variable wake times (especially weekend “catch up” sleep) create circadian desynchrony—essentially giving yourself jet lag every week.
Common objection: “I need to catch up on weekends!”
The reality: Weekend sleep schedule deviation >2 hours creates “social jet lag”—circadian misalignment equivalent to flying across 2-3 time zones and back weekly. This impairs glucose metabolism, increases inflammation, and reduces Monday-Tuesday cognitive performance.
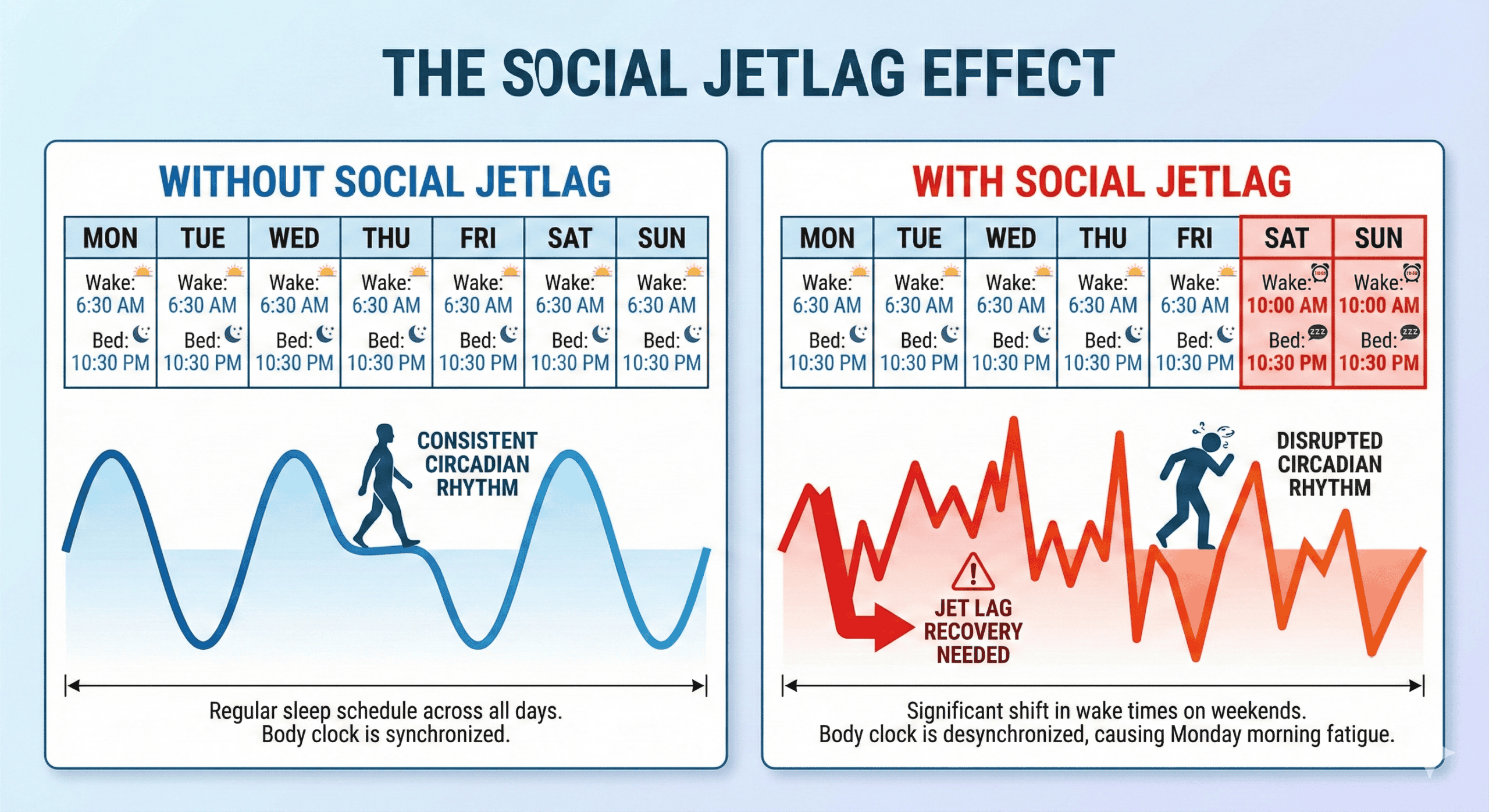 Fig 2.3: Social Jetlag
Fig 2.3: Social Jetlag
Temperature Rhythm: The Forgotten Circadian Tool
Core body temperature follows a circadian rhythm, peaking in late afternoon (~6-7 PM) and reaching lowest point in early morning (~4-5 AM). This rhythm directly influences sleep.
Optimization strategies:
Evening temperature drop acceleration:
- Warm shower/bath 60-90 minutes before bed (paradoxically helps because blood vessels dilate, dumping heat when you exit)
- Cool bedroom (see Pillar 3)
- Avoid intense exercise <3 hours before bed (elevates core temp)
Morning temperature rise:
- Light exercise upon waking
- Morning light exposure (also raises core temp)
- Cool shower → warm progression
- Warm breakfast
Meal Timing and Circadian Rhythm
Food intake is a circadian time cue (though weaker than light). Your digestive system, metabolism, and hormone systems all follow circadian patterns.
Guidelines for circadian optimization:
- Consistent meal timing: Eat meals at roughly the same time daily
- Front-load calories: Larger breakfast/lunch, lighter dinner
- Last substantial meal: 3+ hours before bed (allows temperature drop, reduces digestive interference)
- Avoid late-night eating: Disrupts circadian rhythms, impairs glucose metabolism
Exercise Timing for Circadian Support
Exercise affects circadian rhythm, body temperature, and sleep pressure—making timing strategically important.
Optimal timing windows:
- Morning (6-9 AM): Strengthens circadian rhythm, elevates core temperature (alertness).
- Afternoon (3-6 PM): Physical performance peaks, builds sleep pressure for evening, sufficient time for core temp to drop before bed. Optimal for most people.
- Evening (6-9 PM): Acceptable if finished 3+ hours before bed.
- Intense exercise <2 hours before bed (elevates core temp, cortisol, sympathetic activation)
- Completely sedentary lifestyle (reduces sleep pressure, weakens circadian amplitude)
Pressure Management
Goal: Build adequate homeostatic sleep drive (adenosine accumulation) while avoiding factors that mask or prematurely dissipate it.
Remember Process S: sleep pressure builds linearly from the moment you wake until the moment you sleep. The higher the pressure at bedtime, the faster you fall asleep and the more consolidated your sleep.
Strategic Caffeine Use (The 10-Hour Rule)
Caffeine is an adenosine receptor antagonist. It doesn’t eliminate sleep pressure; it masks it. With a quarter-life of 10-12 hours, a noon coffee means 25% of that caffeine is still blocking deep sleep receptors at midnight. Research shows caffeine consumed even 6 hours before bed reduces sleep quality, though people don’t notice because they “fall asleep fine.”
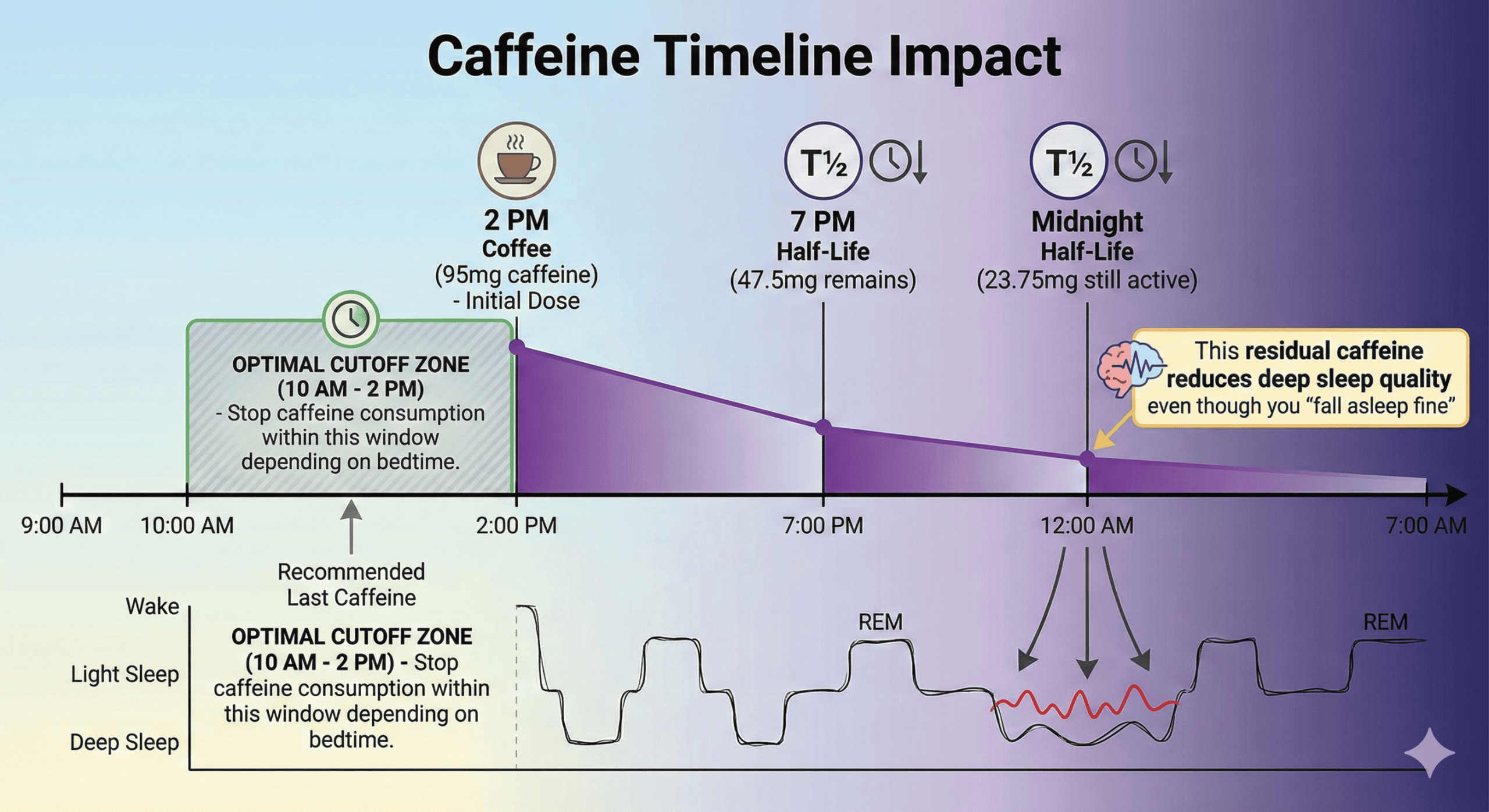 Fig 2.4: Caffeine Half-Life
Fig 2.4: Caffeine Half-Life
Common questions:
- “What about decaf?” → Decaf still contains 2-15mg caffeine per cup. Better than regular, but not zero.
- “I fall asleep fine with afternoon caffeine!” → Your subjective sleep onset doesn’t reflect architecture degradation. Use a sleep tracker or 30-day elimination trial to see the difference in deep sleep %.
Napping Strategy
Naps can be beneficial (increased alertness, learning consolidation) or detrimental (reduced nighttime sleep pressure), depending on timing and duration.
Who should avoid naps: Anyone with insomnia or difficulty falling asleep at night (need maximum pressure). Anyone trying to shift sleep phase earlier.
Sleep Restriction: The Counter-Intuitive Pressure Builder
The paradox: If sleep efficiency is low (<85%), spend less time in bed. Match time-in-bed to actual sleep time to build massive pressure, then gradually extend.
Managing External Sleep Pressure Disruptors
Beyond caffeine, several factors dissipate or interfere with sleep pressure:
- Alcohol: Masquerades as a sleep aid. Severely suppresses REM sleep. Causes fragmentation. Recommendation: Zero alcohol 4+ hours before bed.
- Nicotine: Stimulant effect similar to caffeine. Withdrawal during night causes awakening. Recommendation: Avoid 3+ hours before bed.
- Bright light exposure (evening): Suppresses melatonin, delays circadian phase. Recommendation: Progressive dimming 2-3 hours before bed.
- Mental/emotional arousal: Stress/anxiety elevate cortisol, opposing sleep pressure. Recommendation: Wind-down protocol (Pillar 4).
Recovery Environment Design
Goal: Create sensory and physiological conditions that facilitate rapid sleep onset, minimize sleep fragmentation, and optimize sleep architecture.
Your bedroom environment directly affects sleep onset latency, fragmentation, stage distribution, and overall restoration. Even with perfect circadian alignment and sleep pressure, poor environment degrades architecture.
Temperature: The Deep Sleep Optimizer
The mechanism: Sleep onset requires core body temperature to drop 2-3°F. Deep sleep occurs during the nadir. If ambient temperature is too warm, your body cannot achieve adequate core temperature reduction. Research findings show optimal bedroom temperature is 65-68°F (18-20°C) for most people.
Darkness: The Melatonin Protector
Light exposure during sleep suppresses melatonin and signals “daytime.” Even relatively dim light through closed eyelids reaches the retina. Complete darkness (<5 lux) optimizes melatonin production. Even 8-10 lux during sleep can suppress melatonin ~50%.
The hand test: If you can see your hand in front of your face in your bedroom with all lights off, it’s not dark enough.
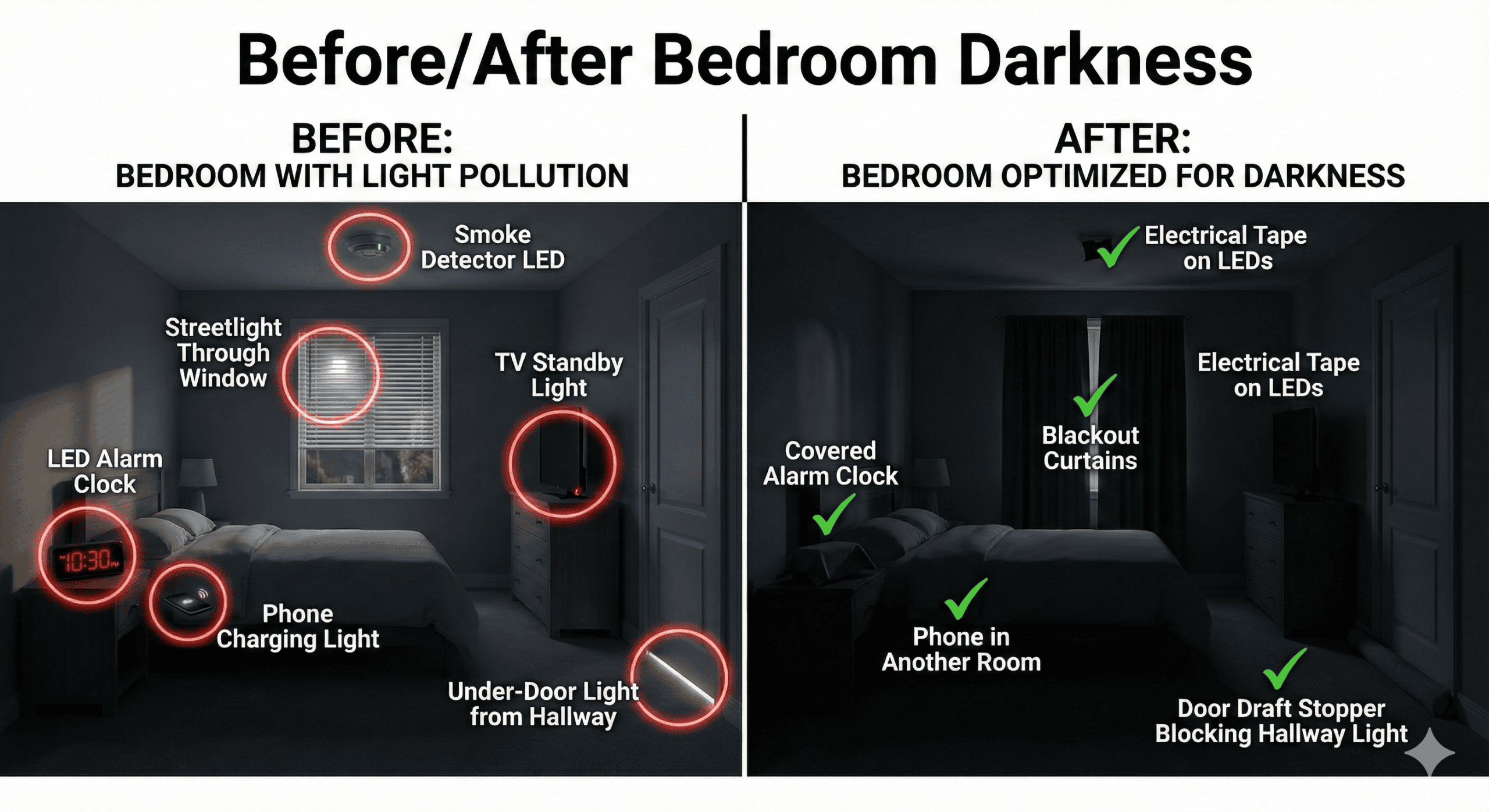 Fig 2.5: Lux Levels
Fig 2.5: Lux Levels
Sound: The Fragmentation Reducer
During sleep, your brain continues processing environmental sounds. Sudden, variable sounds cause micro-arousals that fragment sleep architecture. The solution is sound masking, not elimination.
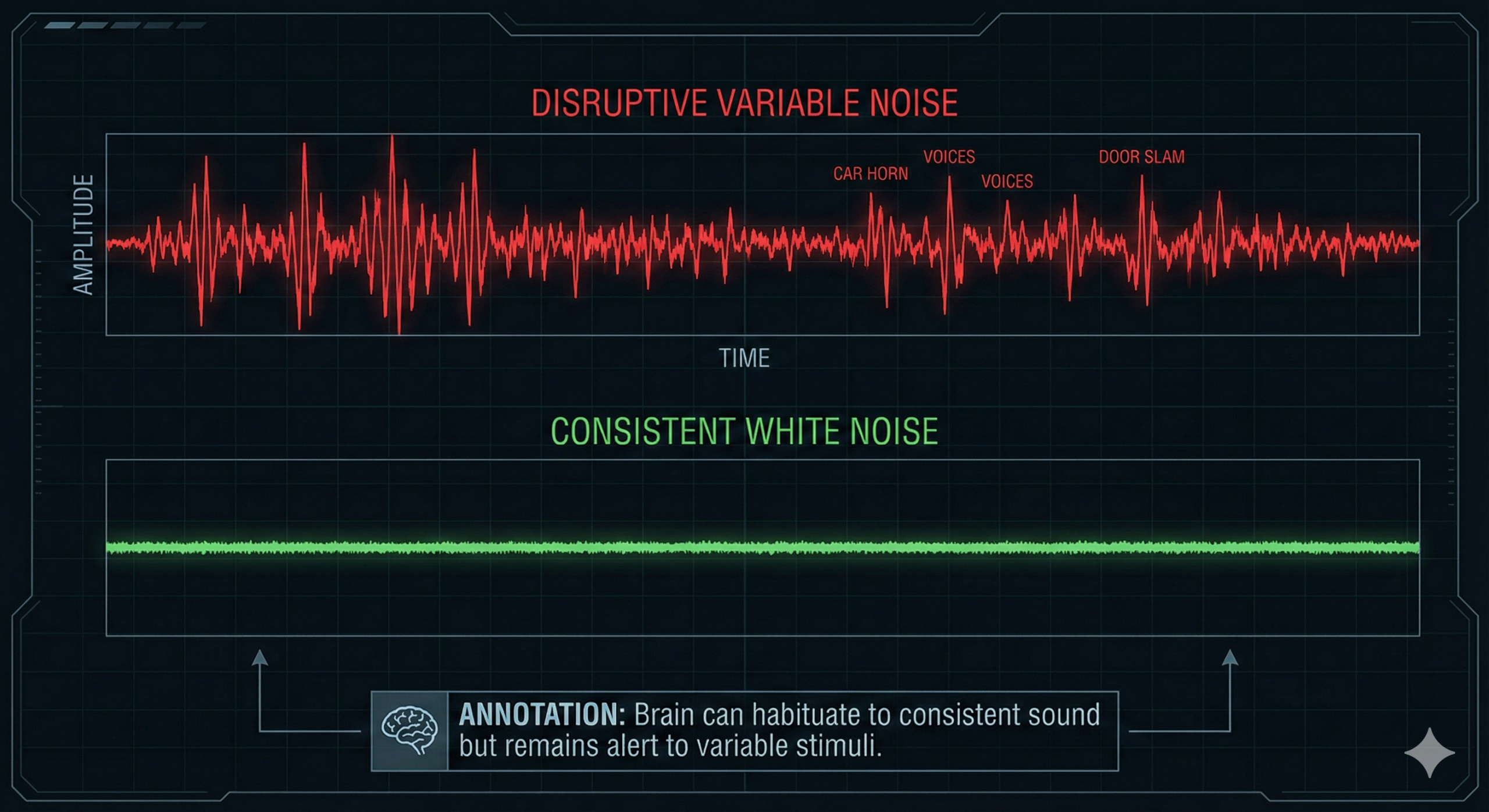 Fig 2.6: Sound Masking
Fig 2.6: Sound Masking
Sound optimization strategies:
- White/Pink/Brown Noise: Consistent background noise masks sudden disruptive sounds. Use a dedicated machine or fan.
- Earplugs: Useful for high-noise environments. Caution: May prevent hearing important sounds like alarms.
- Partner snoring: Evaluate for sleep apnea. Use white noise + earplugs. Consider separate sleep spaces if severe.
Air Quality: The Invisible Performance Factor
You breathe ~7,000-8,000 liters of air during an 8-hour sleep period. Poor air quality (high CO2, low oxygen, pollutants) directly impairs sleep quality and next-day cognitive function.
Implementation:
- Ventilation: Crack window if possible, run HVAC fan, or leave bedroom door open.
- Air purification: HEPA air purifier for pollutants/allergens.
- Humidity management: Keep between 30-50%.
Pre-Sleep Wind-Down Protocol
Goal: Systematically transition from Sympathetic (Alert) to Parasympathetic (Rest) activation. Think of it like landing an airplane—you need a gradual descent.
The 90-Minute Wind-Down Timeline
Why 90 minutes: Research on ultradian rhythms suggests 60-120 minutes is necessary for complete nervous system shift.
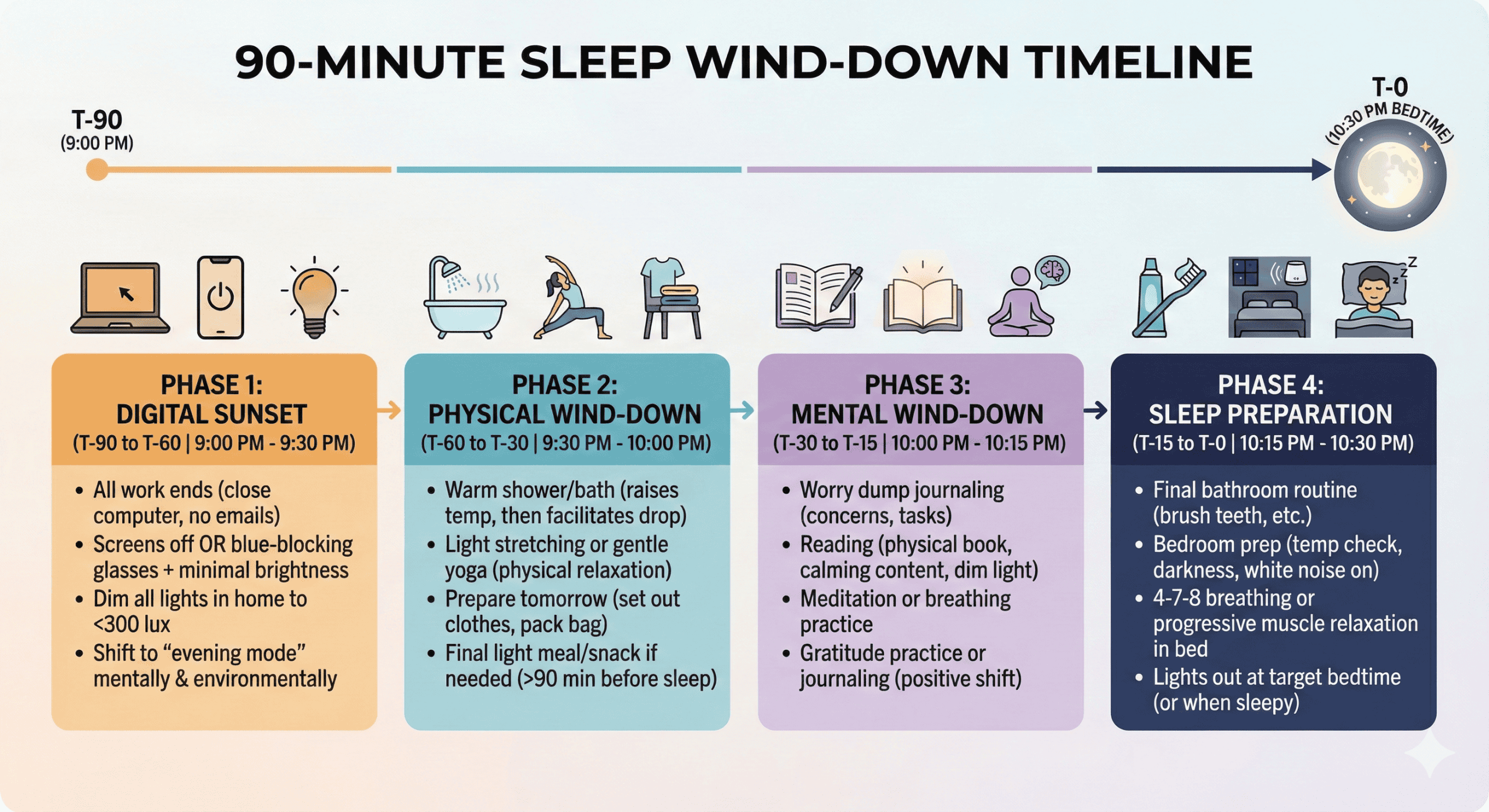 Fig 2.7: The Transition
Fig 2.7: The Transition
The Digital Sunset Protocol
The optimal protocol: Complete screen cessation 90-120 minutes before bed.
The realistic protocol (for those who “must” use screens):
- 60-90 mins before: Enable Night Shift/f.lux (max warmth). Reduce brightness to 20-30%. Wear blue-blocking glasses. Avoid stimulating content (news, work).
- 30 mins before: All screens OFF (no exceptions). Transition to non-digital activities.
Cognitive Wind-Down: The Worry Dump
The problem: Racing thoughts and unfinished mental loops prevent sleep onset. The solution: Externalize all thoughts onto paper.
Physiological Shift: 4-7-8 Breathing
The extended exhale (8 count) activates the Vagus nerve, slowing heart rate and dropping cortisol.
Protocol: Perform while lying in bed, lights out. 4-8 complete cycles. Combine with body scan or progressive muscle relaxation if desired.
Temperature Manipulation for Sleep Onset
The warm bath/shower protocol: Timing: 60-90 minutes before bed. Warm water raises core body temperature; exiting causes vasodilation and rapid heat dump, accelerating the natural drop needed for sleep. Water temp: 104-109°F for 10-20 minutes.
What to AVOID During Wind-Down
- Exercise: Intense exercise <3 hours before bed.
- Stimulating content: News, work email, arguments, intense entertainment.
- Bright light: Overhead lighting, bright screens.
- Stimulants: Caffeine or nicotine.
- Alcohol: “Nightcaps.”
- Large meals: Heavy dinners.
Supplement Stack (Optional)
Note: Supplements are NOT required. Focus on behavioral/environmental factors first.
| Stack | Supplements | Timing | Purpose | Who It’s For |
|---|---|---|---|---|
| Foundational | Magnesium Glycinate (400mg) | 60 min pre-bed | Relaxation, muscle tension | Most people starting supplementation |
| Deep Sleep Optimizer | Mag Glycinate (400mg) + Glycine (3g) | 90 min pre-bed | Deep sleep enhancement, temperature drop | Athletes, hard trainers, deep sleep <15% |
| Circadian Support | Melatonin (0.5-1mg) | 30 min pre-bed | Sleep onset, circadian alignment | Shift workers, travelers, delayed sleep phase |
| Cognitive + Sleep | Mag Threonate (2g) + L-Theanine (200mg) | 60 min pre-bed | Cognitive recovery + relaxation | Knowledge workers, students |
| Comprehensive | Mag Glycinate (400mg) + Glycine (3g) + Apigenin (50mg) | 60-90 min pre-bed | Multi-mechanism optimization | Advanced optimizers after behavioral factors maximized |
Intervention Complexity Matrix
Not sure where to start or what requires the most effort? This matrix ranks all major interventions by implementation difficulty, time requirement, and impact potential.
| Intervention | Difficulty | Time Investment | Cost | Impact | Priority |
|---|---|---|---|---|---|
| Consistent wake time | Easy | 0 min | $0 | ★★★★★ | #1 |
| Phone out of bedroom | Easy | 0 min | $0-20 | ★★★★★ | #2 |
| Morning light exposure | Moderate | 20 min/day | $0-150 | ★★★★★ | #3 |
| Caffeine cutoff 10hr | Easy | 0 min | $0 | ★★★★ | #4 |
| Bedroom cooling | Moderate | 5 min (setup) | $0-500 | ★★★★ | #5 |
| Complete darkness | Easy | 15 min (one-time) | $0-100 | ★★★★ | #6 |
| 90-min wind-down | Difficult | 90 min/day | $0 | ★★★★ | Week 2-3 |
| Digital sunset protocol | Moderate | Part of wind-down | $0-50 | ★★⭐ | Week 2-3 |
| White noise setup | Easy | 5 min (one-time) | $0-100 | ★★⭐ | If noisy |
| Evening light dimming | Moderate | 10 min/day | $0-200 | ★★⭐ | Week 3-4 |
| Blackout curtains install | Moderate | 30-60 min (one-time) | $50-150 | ★★★★ | Week 3 |
| Supplement stack | Easy | 2 min/day | $20-60/mo | ★★⭐ | Week 4+ |
| Sleep tracking device | Moderate | 5 min/day | $200-400 | ★★ | Advanced |
| Mattress replacement | Difficult | 2-4 hours | $500-3000 | ★★⭐ | If needed |
| Cooling mattress pad | Moderate | 15 min (setup) | $500-2000 | ★★★★ | Advanced |
| Bedroom renovation | Difficult | Days-weeks | $1000+ | ★★⭐ | If necessary |
Recommended Implementation Sequence:
- PHASE 1 – FREE & EASY (Week 1): Consistent wake time, Phone out of bedroom, Caffeine cutoff, Tape over LEDs, Temp adjustment. (Effort: <30 min. Impact: 40-50%)
- PHASE 2 – LOW-MODERATE INVESTMENT (Weeks 2-4): Morning light commitment, Blackout solution, White noise, Basic supplements, 90-min wind-down routine. (Effort: 2-3 hrs setup + daily. Cost: $150-400. Impact: +30-35%)
- PHASE 3 – SIGNIFICANT INVESTMENT (Month 2-3+): Smart lighting, Cooling mattress pad, Sleep study, Advanced supplements, Tracking optimization. (Effort: 5-10 hrs + ongoing. Cost: $500-2000+. Impact: +10-15%)
ROI Calculator: Impact by Budget
Focus on: Wake time, phone removal, caffeine rules, morning outdoor light, temp adjustment. (Results: 7-14 days)
Adds: Blackout curtains ($50) + basic supplements ($30) + tape/earplugs ($20). (Results: 14-21 days)
Adds: Light therapy box ($150) + white noise ($100) + quality blackout ($100) + supplements ($50) + blue-blockers ($50). (Results: 21-30 days)
Adds: Cooling mattress pad ($500-2000) + smart bulbs ($150) + Oura/WHOOP ($300-400). (Results: 30-60 days)
Note: The financial investment curve shows diminishing returns. $0-100 provides 60-75% of total benefit, while $2000+ only adds another 10-20% beyond that.
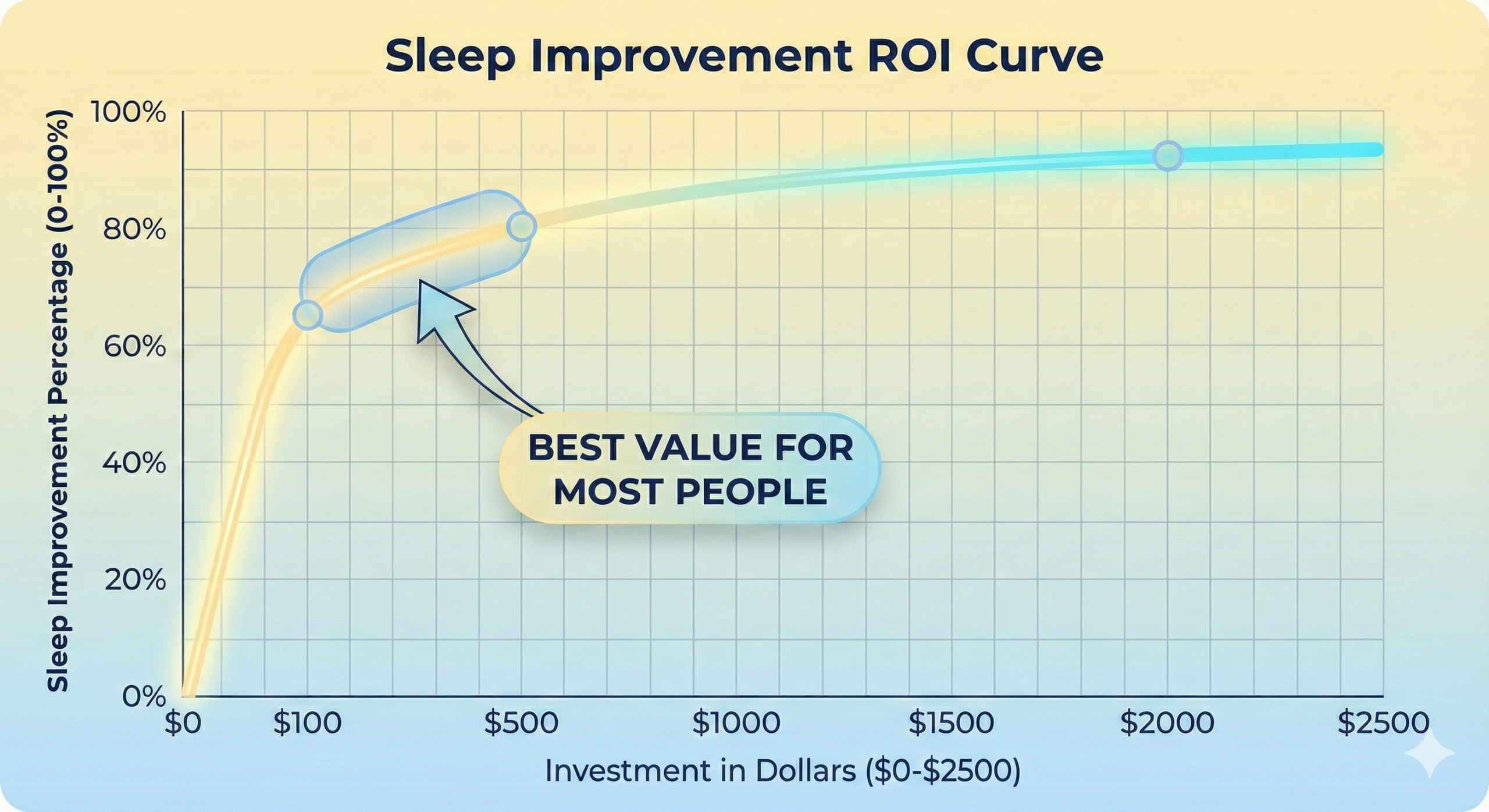 Fig 2.9: The Diminishing Returns Curve
Fig 2.9: The Diminishing Returns Curve
The Sleep Architecture Protocol
A 90-day systematic programme to identify, counteract, and permanently reduce cognitive biases in your decision-making — from individual recognition through organisational transformation to permanent integration.
Based on Kahneman, Tetlock, Klein, and 40+ years of decision science research
Day Complete
Great work on your sleep practice.
Sleep Data Interpretation
Have a sleep tracker (Oura, WHOOP, Apple Watch, Fitbit) but not sure what the data means? This guide teaches you to interpret metrics and take appropriate action.
Understanding Device Accuracy Limitations
Consumer sleep trackers are 60-80% accurate for sleep staging compared to medical polysomnography. Use for trends, not absolute truth.
What trackers measure WELL:
- ✅ Total sleep time (±15 minutes accuracy)
- ✅ Sleep onset time and wake time
- ✅ Movement and restlessness
- ✅ Heart rate and HRV trends
- ✅ Wake-ups (though may miss brief ones)
What trackers measure POORLY:
- ⚠️ Sleep stage classification (30-40% error rate vs. PSG)
- ⚠️ Exact deep sleep vs. light sleep differentiation
- ⚠️ Precise REM timing
How to use data: Compare YOUR nights to YOUR other nights (individual trends). Don't compare to population averages or other people. Look for patterns over 7-30 days, not single nights. Validate against subjective feeling (do you feel restored?).
Key Metrics Decoded
What it is: Time from first sleep onset to final wake.
| Your TST | Interpretation | Action Needed |
|---|---|---|
| < 6 hours | Sleep Deprived | Red Alert: Extend sleep opportunity immediately. Chronic performance impairment. |
| 6-7 hours | Insufficient for most | Yellow: Monitor daytime function. If impaired, extend to 7-8h. |
| 7-9 hours | Optimal range | Green: Maintain current duration if feeling restored. |
| > 9.5 hours | Possibly oversleeping | Yellow: May indicate underlying issue (depression, illness, catching up from debt). Monitor. |
Common pattern: Weekday 6.5h, weekend 9h = Chronic sleep debt + social jet lag. Fix: Consistent 7.5-8h nightly.
What it is: (Total Sleep Time / Time in Bed) × 100.
| Efficiency | Interpretation | Action Needed |
|---|---|---|
| < 75% | Severe fragmentation | Red: Check for sleep disorder (apnea, restless legs). If ruled out, implement stimulus control therapy. |
| 75-85% | Moderate inefficiency | Yellow: Reduce time in bed (sleep restriction), eliminate alcohol, address stress. |
| 85-90% | Good efficiency | Green: Fine-tune with environment optimization. |
| 90-95% | Excellent efficiency | Green: Maintain current practices. |
| > 95% | Possibly excessive pressure | Yellow: Might be sleep deprived. Check if TST is adequate. |
Red flag pattern: Efficiency <80% for >2 weeks despite optimization = Sleep study recommended.
What it is: Percentage of total sleep time spent in N3 stage. (Device accuracy: ~30-40% error rate; use for trends only).
| Your Deep % | Interpretation | Action Needed |
|---|---|---|
| < 10% | Significantly deficient | Red: Eliminate alcohol completely. Drop bedroom temp to 64-65°F. Caffeine cutoff to noon. If no improvement in 30 days → sleep study. |
| 10-15% | Below optimal | Yellow: Optimize temperature, caffeine timing, alcohol. Add glycine supplementation. |
| 15-25% | Optimal range | Green: Maintain current practices. |
| > 25% | Unusually high | Green/Yellow: May indicate recovery from prior debt. Monitor if sustained. |
Common saboteur: Alcohol suppresses deep sleep by 20-40% even 3-4 hours before bed.
Age adjustment: 20-30 years: Target 18-25%. 30-50 years: Target 15-22%. 50-70 years: Target 10-18%. 70+ years: 5-15% may be normal.
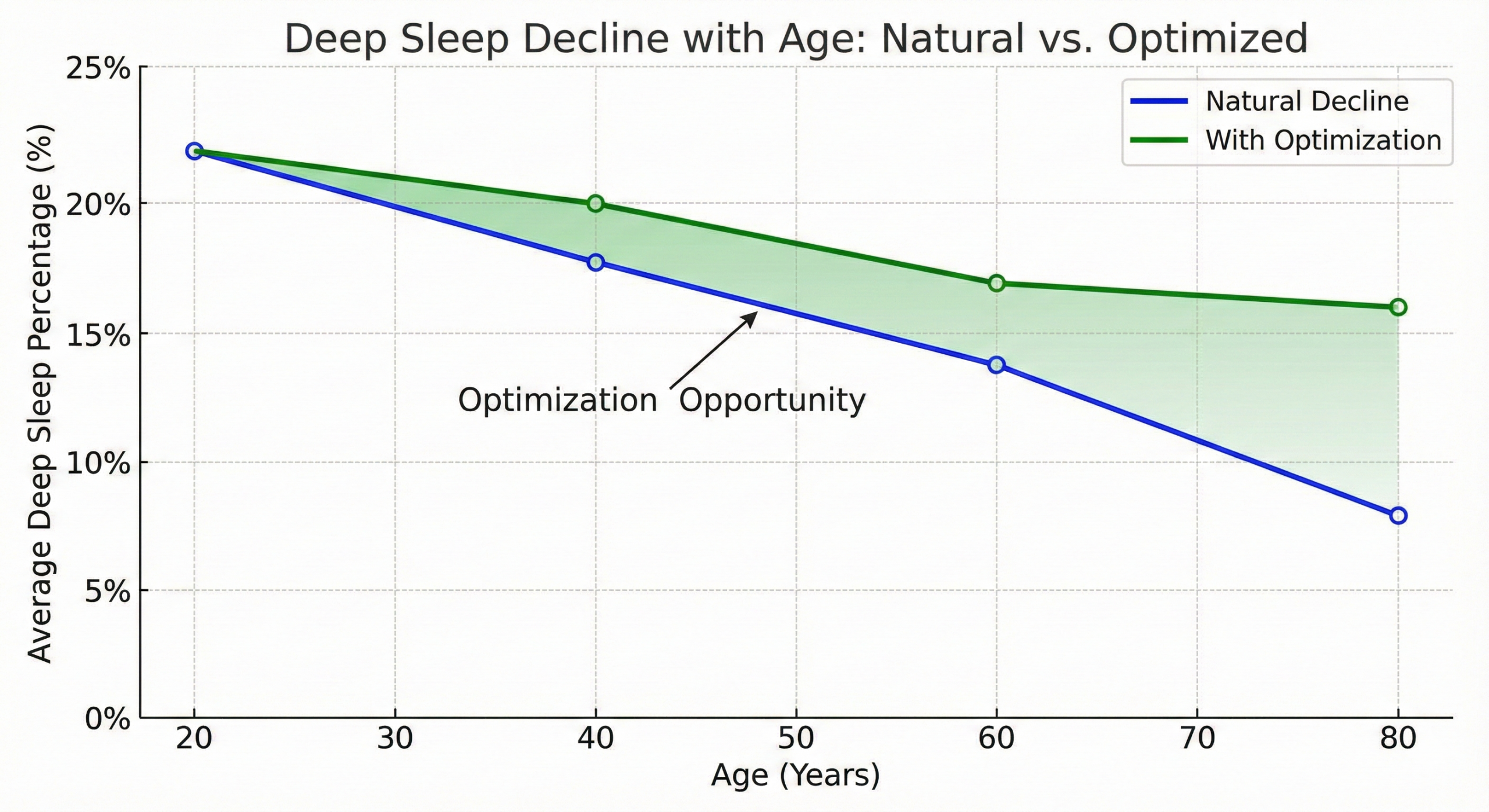 Fig 5.1: Age-Related Decline
Fig 5.1: Age-Related Decline
What it is: Percentage of total sleep time in REM stage. (Device accuracy: ~30-40% error rate; use for trends only).
| Your REM % | Interpretation | Action Needed |
|---|---|---|
| < 15% | Significantly deficient | Red: Eliminate alcohol entirely. Check medications (SSRIs, beta-blockers suppress REM). Protect morning sleep (REM concentrated in final cycles). Sleep study if persistent. |
| 15-20% | Below optimal | Yellow: Avoid sleep restriction. Protect total sleep duration. Address stress (REM processes emotions). |
| 20-25% | Optimal range | Green: Maintain practices. |
| > 25% | Elevated REM | Yellow: May indicate REM rebound from prior suppression, high stress, or medication effect. |
Common saboteur: Cutting sleep short (early alarm) disproportionately eliminates REM-rich final cycles.
Stress impact: Chronic stress can both suppress REM (overwhelm) and increase REM (rebound processing). Monitor stress management.
What it is: Variation in time between heartbeats (higher = better autonomic balance). Healthy range is highly individual (30-100+ ms); compare to YOUR baseline.
| HRV Trend | Interpretation | Action Needed |
|---|---|---|
| Declining for 3+ days | Insufficient recovery | Red: Extend sleep by 30-60 min. Reduce training intensity. Check for illness. Prioritize stress management. |
| Consistently below personal average | Chronic underrecovery | Yellow: Something is wrong. Check: Sleep duration, sleep quality, stress levels, overtraining, illness brewing. |
| At or above personal average | Good recovery status | Green: Current sleep/stress balance is working. |
| Unusually high (>30% above average) | Possible parasympathetic overtraining | Yellow: Can indicate overtraining paradox. Monitor energy and performance. |
Use HRV for decisions: Low HRV morning = Reduce workout intensity, prioritize sleep. High HRV morning = Ready for hard training. Chronic low HRV = Reassess entire recovery protocol.
Warning: HRV decreases naturally with age. Compare to YOUR baseline, not population averages.
What it is: Average heart rate during sleep. Healthy range: 40-70 bpm (athletes lower, varies by fitness).
| RHR Change | Interpretation | Action Needed |
|---|---|---|
| Elevated 5+ bpm for 3+ nights | Stress/illness/overtraining | Red: Check for illness. Extend sleep. Reduce stress/training. |
| Gradual increase over weeks | Declining fitness or increasing stress | Yellow: Assess training load, stress levels, sleep quality, diet. |
| Stable at baseline | Good recovery | Green: Continue current practices. |
| Decreasing over months | Improving fitness | Green: Training is working. |
Red flag: RHR suddenly 10+ bpm above baseline = Possible illness, overtraining, or sleep disorder. Medical evaluation if sustained.
Pattern Recognition: Common Sleep Data Profiles
Deep sleep: 8-12% (low)
Efficiency: 75-85% (moderate)
Latency: 20-40 minutes
Subjective: "I sleep fine, just wake up tired"
What's happening: Caffeine (even 10 hours before bed) suppresses deep sleep architecture. You fall asleep but architecture is impaired.
Fix: Caffeine cutoff to 12 PM or earlier for 2 weeks. Deep sleep should improve to 15-20%.
REM sleep: 10-15% (very low)
Deep sleep: 10-13% (low-normal)
Awakenings: 8-15 (high)
Efficiency: 70-80% (low)
Pattern: Worse on nights with evening drinks.
What's happening: Alcohol sedates (you fall asleep) but destroys REM and fragments sleep as it metabolizes.
Fix: 30-day alcohol elimination trial. REM typically jumps to 20-23%, fragmentation drops dramatically.
Latency: 45-90 minutes (very high)
Total sleep: 6-7 hours despite 8 hours in bed
HR: Elevated during sleep
HRV: Below personal average
Subjective: "Mind won't shut off"
What's happening: Elevated cognitive arousal preventing sleep onset + sympathetic nervous system activation.
Fix: Extended wind-down (120 min), worry dump journaling, 4-7-8 breathing, eliminate screens 2+ hours before bed, consider therapy for anxiety.
Efficiency: <75% with frequent "awake" periods
SpO2 (if tracked): Dips below 90%
Snoring detected
REM/Deep sleep: Both low
Subjective: Exhausted despite "8 hours sleep"
What's happening: Breathing disruptions fragmenting sleep architecture, preventing restorative stages.
Fix: Sleep study immediately. This cannot be optimized behaviorally. Requires medical intervention (CPAP, oral appliance, surgery).
Weekday: 6-6.5h (Eff 85-90%)
Weekend: 9-10h (Eff 90-95%)
Mon/Tue: Poor quality, HRV drops
What's happening: 2-3 hour weekend sleep schedule shift creates circadian misalignment equivalent to flying across time zones weekly.
Fix: Consistent wake time ±30 min every day. If sleep-deprived, go to bed earlier on weekends, not later on weekends.
Data-Driven Decision Making
- Week 1-2: Collect baseline data. Don't change anything, just observe. Note patterns: Which nights are best/worst? What correlates? Identify 1-2 clear issues from profiles above.
- Week 3-4: Test one variable. Change ONLY one thing (e.g., caffeine cutoff). Track for 2 weeks minimum. Compare to baseline. If improved, keep. If not, try different variable.
- Week 5-6: Add second variable. Layer in another optimization. Continue tracking. Assess compounding effects.
- Monthly review: What's working? (keep doing). What's not changing? (try different intervention). What's worse? (revert that change).
When Data Suggests Medical Evaluation
- Efficiency <75% for >4 weeks despite optimization
- Deep sleep <8% consistently with good sleep hygiene
- Suspected apnea pattern (snoring + fragmentation + low SpO2)
- REM <12% for >4 weeks (check medications first)
- HRV chronically low despite adequate sleep duration
- Daytime microsleeps or extreme sleepiness despite 7-9 hours
Don't wait months if severe. Sleep disorders worsen without treatment.
The Sleep Onset Protocol
For those who struggle specifically with falling asleep (sleep onset latency >30 minutes consistently). This protocol addresses the physiological, psychological, and behavioral barriers preventing rapid sleep onset.
Understanding Sleep Onset Mechanisms
Sleep onset isn't a binary switch—it's a gradual transition requiring:
- Adequate homeostatic sleep pressure (adenosine accumulation)
- Appropriate circadian timing (biological night)
- Parasympathetic nervous system activation (relaxation)
- Absence of arousal (physical, cognitive, emotional)
When sleep onset is delayed, one or more of these mechanisms is impaired.
Diagnostic Flowchart: Why Can't I Fall Asleep?
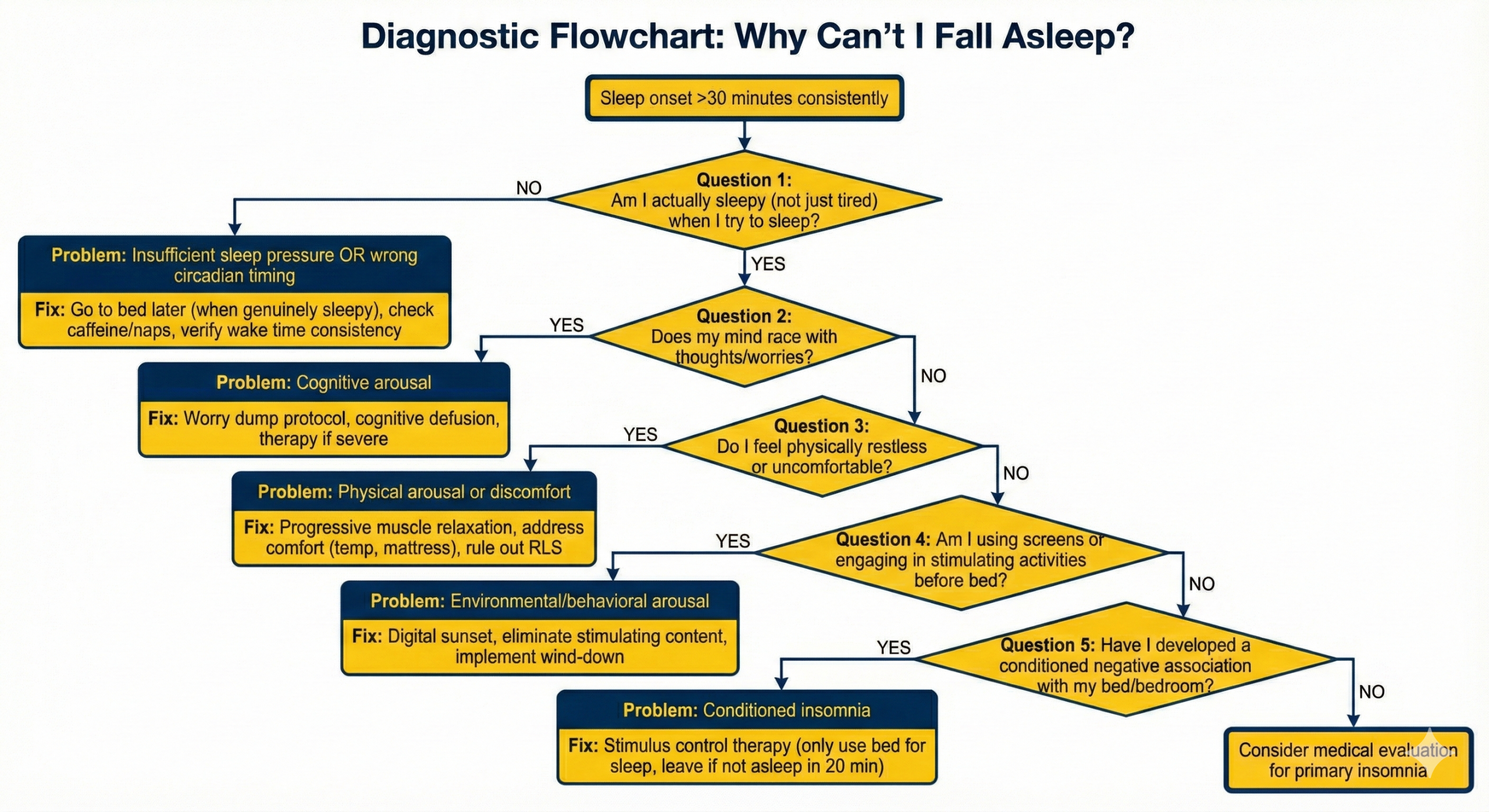 Fig 6.1: Logic Tree
Fig 6.1: Logic Tree
Barrier-Specific Interventions
Sleepiness vs. Fatigue
| State | Symptoms | Action |
|---|---|---|
| Fatigue | Exhausted, "tired," low energy, but can stay awake. | Do NOT go to bed yet. Wind down. |
| Sleepiness | Heavy eyelids, yawning, nodding off, fighting to stay open. | Go to bed immediately. |
The Solution: Wait for genuine sleepiness before bed, even if late. Sleep pressure will build, and circadian rhythm will adjust.
The Complete Sleep Onset Protocol
During the Day
- Consistent wake time (builds anchor).
- Morning light exposure.
- Caffeine cutoff 10 hours before bed.
- Physical activity. No naps.
Evening Sequence
- 3 Hours Before: Last meal. Begin dimming.
- 90 Mins Before: Screens OFF. Worry Dump (15 min).
- 60 Mins Before: Warm shower. Light stretch. Prepare tomorrow.
- 30 Mins Before: Quiet reading. Lights <50 lux.
- Bedtime: Only enter when sleepy. 4-7-8 Breathing.
- Fail-Safe: If not asleep in 20 min → GET UP.
- Week 1: May get up multiple times (breaking old patterns).
- Week 2: Getting up less frequently, sleep onset improving.
- Week 3-4: Sleep onset typically <20 minutes, association rebuilt.
Sleep Maintenance & Architecture
For those who fall asleep fine but wake frequently or have poor sleep architecture despite adequate duration.
Understanding Sleep Fragmentation
Sleep fragmentation (frequent awakenings) degrades architecture even if total sleep time is adequate. Each awakening disrupts sleep cycle progression, reduces time in restorative stages (deep sleep, REM), impairs memory consolidation, and reduces recovery quality.
Causes of fragmentation: Environmental (sound, light), Physiological (apnea, bladder), Hormonal (cortisol, blood sugar), Behavioral (alcohol, caffeine).
Fragmentation Pattern Diagnosis
When you wake during the night matters:
Environmental Causes and Solutions
Physiological Causes and Solutions
Signs: Loud snoring, gasping/choking, daytime sleepiness, morning headaches, high blood pressure.
Impact: Causes dozens to hundreds of micro-arousals per night. Prevents deep sleep/REM. Serious cardiovascular consequences.
Action: Home sleep test or In-lab polysomnography. Treatment: CPAP, oral appliance. Do not attempt behavioral optimization if apnea is present.
Causes: Fluid too close to bed, diuretics, apnea, prostate issues.
- Solutions: Stop fluids 2+ hours before bed. Empty bladder immediately before bed. Reduce evening alcohol/caffeine.
Mechanism: High-carb meal → spike → insulin crash 3-4h later → cortisol release → awakening.
- Signs: Wake 3-4 hours after carb-heavy dinner, feeling anxious/hungry.
- Solutions: Dinner 3+ hours before bed. Moderate protein+fat. Small snack if needed (protein + complex carb).
Pattern: Cortisol should be low at night. Dysregulation causes spikes (often 2-4 AM).
- Signs: Wake same time each night, feel wired/alert, mind racing.
- Solutions: Daytime stress management. Extended wind-down (120 min). Magnesium/Ashwagandha.
Behavioral/Substance Causes
Alcohol (Even Hours Before)
Mechanism: Initial sedation → Metabolism 3-4 hours later → Rebound awakening. Suppresses REM.
Solution: 30-day complete elimination. Long-term: 4+ hours before bed minimum.
Residual Caffeine
Mechanism: Quarter-life 10-12 hours. Afternoon caffeine increases fragmentation.
Solution: Cutoff to noon or earlier. 14-day elimination trial.
Conditioned Arousal (The 3 AM Wake)
Pattern: Brain learns "3 AM = Wake Up."
Solution (Stimulus Control): When you wake, do NOT check the clock. Wait 15-20 mins. If not asleep, GET UP. Do calm activity in dim light. Return only when sleepy.
Architecture Optimization
Even without obvious awakenings, architecture can be suboptimal (low deep/REM %).
Deep Sleep Optimization
- Temperature: Cool bedroom (62-68°F).
- Timing: Protect hours 0-3 (Early night).
- Substances: Eliminate alcohol. Caffeine cutoff.
- Protocols: Glycine (3-5g). Sauna 4-7 hours before bed.
REM Optimization
- Duration: Protect late night (hours 5-8). Don't cut sleep short.
- Substances: Alcohol elimination (crucial). Check meds (SSRIs).
- Protocols: Stress management. Choline supplementation.
Tracking: Use wearable to measure deep/REM %. Track trends over 7-30 days. Target: Deep 15-25%, REM 20-25%.
Special Populations & Tactical Protocols
Sleep optimization isn't one-size-fits-all. These populations face unique challenges requiring adapted protocols.
The challenge: Rapid time zone changes faster than circadian rhythm can adapt (1 day per zone typically).
Jet Lag Minimization Protocol
- Pre-travel (2-3 days): Shift schedule 15-30 min/day toward destination. East=Earlier, West=Later.
- Flight: No alcohol. Hydrate. Sleep if night at destination; stay awake if day.
- Arrival Day: Immediate outdoor light (critical). Stay awake until destination bedtime. Light exercise.
- First 2-3 Nights: Melatonin 0.5-3mg at bedtime. Maintain hygiene.
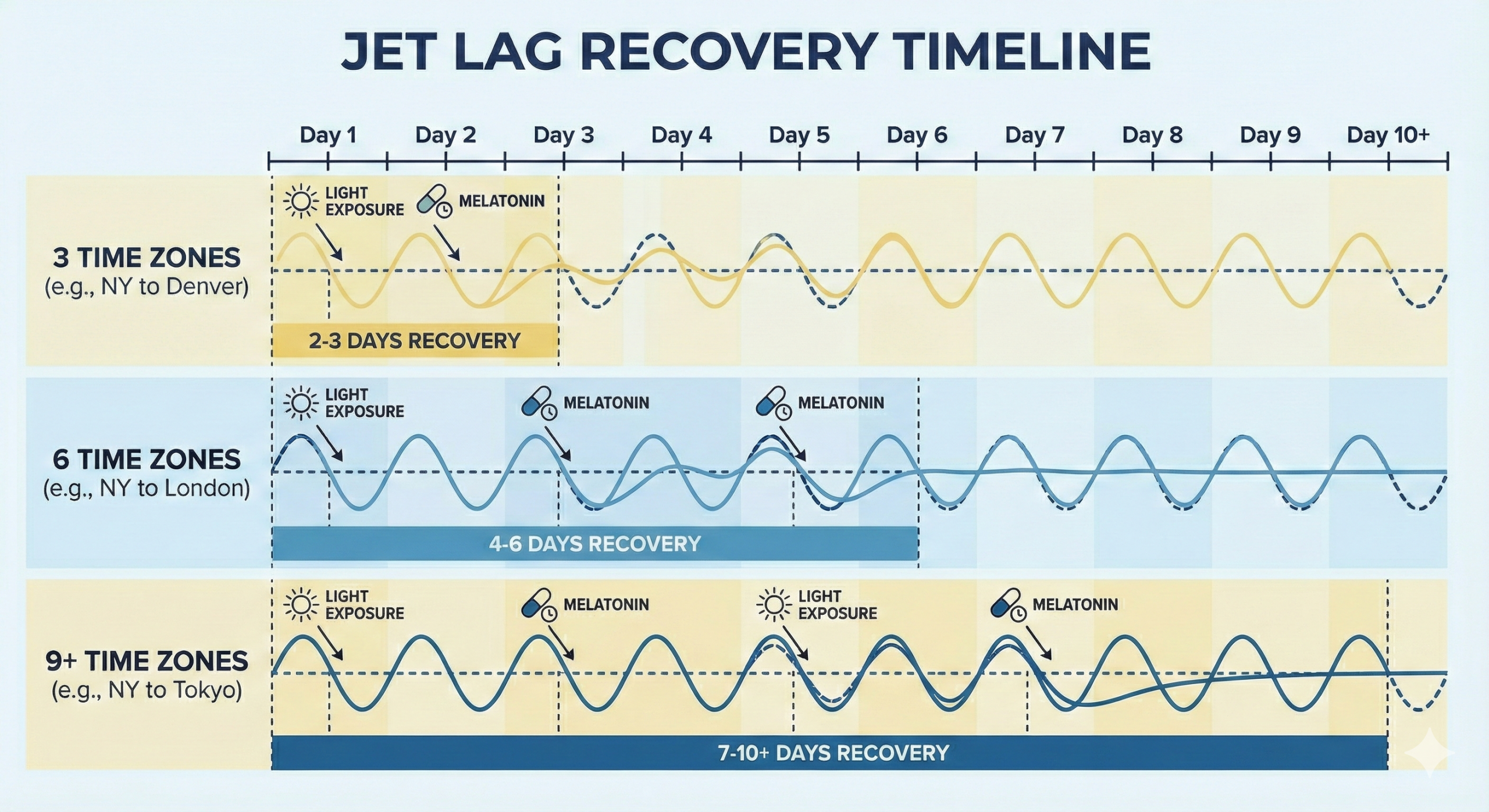 Fig 8.1: Recovery Timeline
Fig 8.1: Recovery Timeline
| Direction | Strategy | Recovery (6hr shift) |
|---|---|---|
| East (Harder) | Advance Phase (Bed Earlier). Morning light at destination essential. | ~5-6 Days |
| West (Easier) | Delay Phase (Stay up later). Evening light helpful. | ~3-4 Days |
Domain-Specific Quick-Start Protocols
One-page protocols adapted for specific situations.
- Hard Shutdown: Alarm at 9:30 PM. Commit work. Close IDE.
- Strict Blue Light: f.lux max warm. Glasses after 8 PM.
- Caffeine Architecture: Track mg. Hard cutoff 11 AM.
- Mental Shutdown: 30-min brain dump (paper only).
- Morning Sun: 15 min walk before opening laptop.
- Light: Bright light first 4h. Blue-blockers last 3h.
- Bedroom: Military blackout. White noise. "Do Not Disturb" sign.
- Melatonin: Strategic use before day-sleep (consult MD).
- Schedule: Request blocks/clusters. 48h recovery post-shift.
- Priority: Protect duration as life-or-death.
- Shifts: Split night 10-2 / 2-6. Off-duty parent leaves room.
- Nap: Sleep when baby sleeps (immediately).
- Environment: Blackout/White noise in both rooms.
- Weekend: One parent gets full night sleep (swap weekly).
- Standard: Lower bar to survival (6h total).
- Calendar: Block 8h sleep. Meeting end 7 PM max.
- Travel: Sleep kit. Shift 2 days prior. Arrival light.
- Sunset: Email auto-reply 8 PM. Phone to assistant.
- Worry Mgmt: 20 min end-of-day brain dump.
- Delegation: Assistant protects sleep schedule.
- No All-Nighters: Study till 12, sleep 7h > Study till 2, sleep 4h.
- Dorm: Eye mask + earplugs + bed tent.
- Boundaries: Socialize weekends only.
- Exams: 8h sleep week prior. Bed 10 PM night before.
- Caffeine: Stop by 2 PM. No energy drinks.
GPAs: Research shows students averaging 7-8 hours sleep have 0.3-0.5 higher GPA than those averaging 6 hours. Sleep is studying. For executives, ROI on 2 hours of sleep vs. impaired work is 300-500%.
Risks & Limitations
Risks, Limitations
& The Dark Side
Where sleep optimisation fails — and the costs of treating rest like a performance metric
You did everything right. Blackout curtains drawn, phone charging in another room, bedroom cooled to 18°C, magnesium taken ninety minutes ago. And now you're lying in the dark, wide awake, mentally auditing whether tonight's sleep will be good enough to protect tomorrow's performance. This is the central paradox of sleep optimisation: the harder you try, the worse it gets. Rest demands surrender, and surrender is the one thing high performers are worst at. Every technique in this guide can improve your sleep — and every one of them can destroy it if applied with the wrong mindset.
Understanding where sleep optimisation breaks down prevents the common trap of making sleep worse through the very techniques designed to improve it. What follows is an honest accounting of the costs, the limits, and the people for whom aggressive sleep engineering does more harm than good.
Where Sleep Optimisation Fails
These failure modes affect anyone who pursues sleep optimisation. But for some, the risks are categorically different.
Who Should Not Use This Approach
Which of these describes you? Honest self-assessment is the first act of sleep optimisation.
Critical Warning
The Nocebo Effect in Sleep Optimisation
Here is the cruellest irony of this entire guide: learning about the devastating effects of poor sleep can make your sleep worse. When you understand that sleep deprivation impairs cognition by 40%, increases cardiovascular risk, and accelerates neurodegeneration, a single bad night becomes terrifying rather than trivial. This is the nocebo effect applied to sleep — negative expectations producing negative outcomes. Research shows that simply believing you slept poorly impairs next-day cognitive performance, independent of actual sleep quality.
Self-Assessment — Check Any That Apply
- A "bad" sleep score on your tracker ruins your mood before you assess how you actually feel
- You lie awake worrying about not sleeping, which prevents you from sleeping
- You avoid social events because they might disrupt your sleep schedule
- You believe one night of poor sleep will significantly harm your health
Protection Against Sleep Anxiety
- Accept that 1–2 poor nights per month is biologically normal — not a crisis requiring intervention
- Never check your sleep tracker immediately upon waking — assess subjective energy first
- Maintain social flexibility — the cortisol cost of isolation exceeds the circadian cost of one late night
- Remember: you are not fragile — humans evolved sleeping on the ground with predators nearby
Failure modes and exclusions describe individual risks. But the deepest limitations aren't personal — they're structural. This is the Sleep Architecture field guide.
The Limits of Individual Sleep Optimisation
Most consequential sleep problems are driven by societal and environmental factors that individual protocols cannot overcome.
If you lead a team, manage a household, or influence workplace policy, these structural interventions address what individual optimisation cannot.
System-Level Solutions
- Implement "no-send" email policies after 8pm and before 7am — protecting employee sleep is a measurable productivity intervention, not a perk
- Advocate for flexible start times — chronotype variation means a 7am meeting is biologically 4am for evening types, destroying their sleep architecture
- Design office lighting with circadian awareness — bright, blue-enriched light in the morning, warmer tones after 2pm, supporting rather than disrupting the hormonal cascade
- Normalise napping infrastructure — a 20-minute post-lunch nap improves afternoon performance by 34% and is standard practice in high-performance military and medical environments
- Address the commute — every 30 minutes of commute time correlates with 10 minutes less sleep; remote work policies are sleep interventions by another name
The goal was never perfection. It was better rest, more consistently — with the wisdom to stop optimising and simply close your eyes.
The risks of sleep optimisation are real: orthosomnia, schedule rigidity, environment dependency, and above all, the nocebo effect that turns sleep knowledge into sleep anxiety. Trust your biology. It knew how to sleep long before you read this guide.
Your Questions Answered
16 research-backed answers covering sleep science, common problems, and optimization strategies — from understanding your sleep architecture to engineering peak recovery.
No questions match your search
Try different keywords or
01What is sleep architecture and why does it matter more than hours in bed?
Sleep architecture is the structured sequence of distinct brain states — N1, N2, N3 (deep), and REM — repeating in approximately 90-minute cycles throughout the night, and its quality determines your cognitive performance far more than total time in bed.
When researchers study sleep using polysomnography, they don't see a uniform state. They observe a highly structured progression where each stage serves completely different restorative functions. Deep sleep (N3) handles physical repair, growth hormone release (80% of daily total), and glymphatic waste clearance. REM sleep handles emotional regulation, creative integration, and procedural memory consolidation. You can spend 9 hours in bed with fragmented architecture and wake exhausted, or spend 7 hours with optimised architecture and wake at 95% cognitive capacity. The critical insight: early cycles are deep-sleep dominant (physical repair), while late cycles are REM dominant (cognitive repair). Cutting sleep short disproportionately eliminates REM.1The memory function of sleepNature Reviews Neuroscience, 11(2), 114–126.2National Sleep Foundation's sleep quality recommendationsSleep Health, 3(1), 6–19.
Two executives both sleep 11pm to 6am. Executive A has fragmented architecture from alcohol and 74°F room: 8% deep, 12% REM. Executive B has optimised conditions: 22% deep, 24% REM. Same duration, dramatically different performance. The difference isn't hours — it's architecture.
Stop counting hours. Start engineering the quality and distribution of your sleep stages.
02What does each sleep stage actually do?
Each of the four sleep stages serves a distinct biological function: N1 is your gateway to sleep, N2 consolidates memories via sleep spindles, N3 (deep sleep) handles physical repair and brain waste clearance, and REM processes emotions and builds creative connections.
Stage N1 (5% of night) is brief transition where sensory input disengages. Stage N2 (45–55%) produces sleep spindles (12–14 Hz bursts) transferring information from hippocampus to neocortex. Stage N3 (15–25%) generates slow delta waves during which growth hormone peaks, immune system strengthens, and the glymphatic system activates. REM (20–25%) mimics waking brain activity — emotional memories process, procedural skills consolidate, and novel associations form.1Sleep, memory, and plasticityAnnual Review of Psychology, 57, 139–166.2About sleep's role in memoryPhysiological Reviews, 93(2), 681–766.
A medical student needs strong N2 and REM for learning. A CrossFit athlete needs deep N3 for recovery. Both need all stages, but their performance bottleneck differs.
All four stages are essential but serve different masters. Understanding this lets you diagnose exactly which stage is underperforming.
03What is the glymphatic system and why is it critical?
The glymphatic system is your brain's waste clearance mechanism — during deep sleep, brain cells physically shrink by approximately 60%, allowing cerebrospinal fluid to flood through and flush out neurotoxic proteins including beta-amyloid and tau.
Discovered in 2013, the glymphatic system operates almost exclusively during deep sleep. CSF flows through channels alongside blood vessels, entering interstitial spaces when neurons shrink. This flow carries away metabolic waste. The system is 60% more active during sleep versus wakefulness. No caffeine, meditation, or supplementation can substitute for the physical fluid dynamics of glymphatic clearance.1Sleep drives metabolite clearance from the adult brainScience, 342(6156), 373–377.2Garbage truck of the brainScience, 340(6140), 1529–1530.
Imagine never taking rubbish out of your house. After one missed collection, barely noticeable. After months, the environment becomes toxic. That's what happens when you chronically shortchange deep sleep.
The glymphatic system only operates during deep sleep. There is no workaround.
04How do the two sleep processes (S and C) control when I sleep?
Two independent systems govern your sleep: Process S (sleep pressure) is a rising tide of adenosine that builds the longer you're awake, and Process C (circadian rhythm) is a 24-hour clock driven by light that determines when your brain expects to sleep.
Adenosine accumulates throughout the day — caffeine blocks these receptors, masking pressure without clearing it. Process C is controlled by the SCN and driven primarily by light exposure, orchestrating temperature, cortisol, and melatonin. Optimal sleep occurs when both align: high adenosine coinciding with the circadian low point. When misaligned (jet lag, shift work), sleep quality collapses even with adequate duration.1The two-process model of sleep regulation: a reappraisalJournal of Sleep Research, 25(2), 131–143.2Contribution of the circadian pacemaker and the sleep homeostat to sleep propensityNeuroscience, 26(4), 1185–1194.
A night-shift worker sleeping 8am–4pm gets 8 hours, but their circadian clock signals "wake up" the entire time. Deep sleep drops 30–40% and REM fragments. Same duration, dramatically worse architecture.
Build adequate sleep pressure (avoid late naps/caffeine), then align with your circadian rhythm through consistent light and timing.
05Why does cutting sleep by 2 hours disproportionately destroy REM?
Sleep cycle composition changes dramatically across the night — early cycles are deep-sleep dominant while late cycles are REM dominant — so cutting your last 2 hours eliminates the richest REM period.
Cycles 1–2 (first 3 hours) are dominated by deep N3 sleep. Cycles 4–5 (final 2–3 hours) contain extended REM periods lasting 30–60 minutes each. If you sleep 6 instead of 8 hours, you lose 60–90% of REM but retain most deep sleep. This explains why short sleepers report physical recovery feels "adequate" but mood, creativity, and learning deteriorate.1Normal human sleep: an overviewPrinciples and Practice of Sleep Medicine (5th ed.).2The cumulative cost of additional wakefulnessSleep, 26(2), 117–126.
A product manager sleeping 6 hours misses the 45-minute REM period in cycle 5. Over a week, she accumulates a 4-hour REM deficit, manifesting as irritability and creative block — REM deprivation symptoms, not "stress."
The last 2 hours aren't optional padding — they contain the majority of your REM sleep.
06Am I really a "short sleeper" or just adapted to impairment?
Less than 1% of the population carries the DEC2 gene mutation for genuine short sleep — the vast majority who claim to function on 5–6 hours have simply lost the ability to perceive their own impairment.
Subjective sleepiness ratings stabilise after 3 days of restriction, but objective cognitive performance continues declining linearly. Two weeks of 6-hour sleep equals 24 hours of total deprivation — yet subjects report feeling "fine." The test: take 2 weeks unrestricted sleep. If you sleep 8–9 hours when allowed, you're chronically restricted.1The transcriptional repressor DEC2 regulates sleep lengthScience, 325(5942), 866–870.2The cumulative cost of additional wakefulnessSleep, 26(2), 117–126.
A hedge fund manager sleeping 5 hours takes a 2-week holiday, sleeps 9 hours nightly for 5 nights, then settles at 7.5. Back at work with 7.5 hours: "Like getting glasses for the first time — I didn't know how blurry everything had been."
Unless genetically tested for DEC2, assume you need 7–9 hours. Sleep deprivation erases your ability to recognise you're impaired.
07Can I catch up on sleep during weekends?
Chronic sleep debt cannot be fully repaid in two days — shifting your schedule by more than 2 hours creates "social jetlag" equivalent to flying 3 time zones every week.
Sleeping until noon Saturday after midnight bedtimes resets your circadian clock late. Sunday night you can't sleep at midnight, starting Monday already in deficit. Social jetlag increases inflammation, impairs glucose metabolism, and correlates with higher BMI. The fix: go to bed earlier while maintaining consistent wake time (±30 minutes).1Social jetlag: misalignment of biological and social timeChronobiology International, 23(1–2), 497–509.2Social jetlag and obesityCurrent Biology, 22(10), 939–943.
A lawyer sleeps midnight–6am weekdays, 2am–11am weekends. Her clock is confused; Monday feels like jet lag until Wednesday. Going to bed at 10pm Friday/Saturday while waking at 6:30am would produce far superior recovery.
Protect your wake time. If in debt, go to bed earlier — never sleep later.
08Why does alcohol ruin my sleep even though it helps me fall asleep?
Alcohol is a sedative, not a sleep aid — it sedates your cortex while fragmenting architecture, suppressing REM by 20–40%, and causing rebound wakefulness when it metabolises around 3–4am.
Alcohol enhances GABA, feeling relaxing, but sedation and sleep are neurologically distinct. During the first half, it may increase deep sleep slightly, but completely disrupts the second half. As the liver metabolises alcohol, rebound sympathetic activation triggers increased heart rate, sweating, and cortisol. Even 1–2 drinks suppress REM 20% and increase fragmentation 30–50%.1Alcohol and sleep I: effects on normal sleepAlcoholism: Clinical and Experimental Research, 37(4), 539–549.2Alcohol and the sleeping brainHandbook of Clinical Neurology, 125, 415–431.
Wearable data from a 35-year-old: on nights with 2 glasses of wine, resting HR +12 BPM, HRV -30%, deep sleep 21%→14%, REM 23%→15%. After 30 days alcohol-free, sleep efficiency improved from 76% to 91%.
The 30-day alcohol-free test is the single most illuminating sleep experiment most people will ever run.
09I can't fall asleep — what's actually going on?
Difficulty falling asleep typically stems from insufficient sleep pressure (adenosine), a hyperactive sympathetic nervous system, or conditioned wakefulness from using your bed for non-sleep activities.
Sleep onset requires convergence of three conditions: adequate adenosine (no late caffeine or naps), parasympathetic dominance (calm physiology), and conditioned bed-sleep association. Caffeine after noon blocks adenosine. Screens and rumination keep the sympathetic system dominant. TV in bed conditions wakefulness. The clinical fix: stimulus control — only go to bed when genuinely sleepy; if not asleep in 20 minutes, get up.1Understanding and treating insomniaAnnual Review of Clinical Psychology, 7, 435–458.2A cognitive model of insomniaBehaviour Research and Therapy, 40(8), 869–893.
A developer lying in bed 90 minutes nightly: caffeine at 4pm, laptop in bed until 11pm, then "trying hard" to sleep. Three changes — noon caffeine cutoff, laptop banned from bedroom, 20-minute rule — dropped onset from 90 to 15 minutes within two weeks.
Stop trying harder to sleep. Remove the obstacles and the nervous system will do what it's designed to do.
10What is the ideal bedroom environment for sleep?
Three non-negotiable parameters: temperature 65–68°F (18–20°C), complete darkness (0–5 lux), and minimal noise disruption.
Your body must drop core temperature 2–3°F to initiate sleep. A cool room facilitates this. Even 8 lux of ambient light suppresses melatonin. Every LED matters. Consistent background sounds mask disruptive spikes. Remove all screens — even a powered-off smartphone reduces sleep efficiency through psychological association.1Effects of thermal environment on sleepJournal of Physiological Anthropology, 31(1), 14.2Effects of artificial light at night on human healthChronobiology International, 32(9), 1294–1310.
One executive covered LEDs with tape, moved phone charger to hallway, lowered thermostat from 72°F to 67°F, added blackout curtains. Sleep efficiency: 78%→92% in one week. Cost: under $50.
Cool, dark, quiet. If you can see your hand, it's not dark enough. If you feel warmth, it's not cool enough.
11How important is consistent wake time?
A consistent wake time (±30 minutes, including weekends) is the single highest-leverage sleep intervention — it anchors your entire circadian rhythm and matters more than bedtime.
Your SCN learns to begin cortisol awakening at 6:30am for a 7am wake time, schedule melatonin onset 14–16 hours later, and organise temperature rhythms. Variable wake times create chronic jet lag. Bedtime naturally adjusts once wake time is fixed through consistent morning light exposure.1Stability, precision, and near-24-hour period of the human circadian pacemakerScience, 284(5423), 2177–2181.2Irregular sleep/wake patterns and academic performanceSleep, 40(6), zsx069.
A consultant with erratic hours tried every supplement. Nothing worked because wake time varied 5:30am to 9am. Fixing it at 6:30am (even weekends) improved sleep efficiency from 74% to 88% in two weeks. The anchor was the fix.
Fix your wake time first. This one commitment has more support than any other sleep intervention.
12How should I time caffeine to protect sleep?
Caffeine's quarter-life is 10–12 hours — 25% of a noon coffee is active at midnight. Evidence-based cutoff: 10 hours before bed minimum. Delay first cup 90–120 minutes after waking.
Caffeine consumed 6 hours before bed still reduces total sleep by 1+ hour and decreases deep sleep — even when subjects report falling asleep "normally." Delaying first intake allows the cortisol awakening response to clear overnight adenosine naturally, producing more sustained alertness and reducing tolerance.1Caffeine effects on sleep taken 0, 3, or 6 hours before going to bedJCSM, 9(11), 1195–1200.2Effects of caffeine on sleep qualityRisk Management and Healthcare Policy, 11, 263–271.
A project manager shifted first coffee from 6:30am to 8:30am and last coffee from 3pm to 12:30pm. Deep sleep: 12%→19% in one week. More alert despite same total caffeine.
Delay first coffee 90 minutes. Cut off 10 hours before bed.
13Do sleep trackers actually work?
Consumer wearables are reasonably accurate for total sleep time and efficiency but significantly less reliable for stage classification — use them for trends, not absolute percentages.
Wearables achieve 80–90% accuracy for sleep vs wake but only 50–65% for distinguishing stages. The real value is relative trends: is deep sleep increasing? Is HRV trending up? The risk is "orthosomnia" — anxiety about data that paradoxically worsens sleep.1Wearable sleep technology in clinical and research settingsMSSE, 51(7), 1538–1557.2OrthosomniaJCSM, 13(2), 351–354.
A fitness enthusiast anxiously checking Oura Ring nightly created anticipatory stress that degraded sleep. Switching to weekly averages resolved both the anxiety and the metrics.
Use trackers for weekly trends, not nightly scores. If tracking creates anxiety, stop for a month.
14What 3 changes should I make tonight?
Tonight: remove phone from bedroom, drop room temperature to 65–68°F, and cover every LED. These require zero willpower and produce measurable improvement on night one.
Phone removal eliminates blue light and notification arousal. Temperature reduction facilitates core body temperature drop. Darkness preserves melatonin. Combined, they create a compounding effect immediately.1Brain drain: smartphone presence reduces cognitive capacityJACR, 2(2), 140–154.2Thermal environment and sleepJPA, 31(1), 14.
47 executives made only these three changes for one week. Average sleep efficiency: 79%→88%. Onset latency: -14 minutes. Morning alertness: +22%. No supplements, no apps.
Phone out, temperature down, lights eliminated. Highest-return, lowest-effort interventions in sleep science.
15What is the optimal wind-down routine?
Your nervous system can't transition instantly from sympathetic to parasympathetic — a 90-minute staged wind-down (T-90, T-60, T-30, T-15) produces the most reliable sleep onset.
T-90: dim lights below 300 lux, screens off. T-60: warm shower (subsequent cooling aids temperature drop), worry-dump journal. T-30: bedroom ready, light fiction reading. T-15: 4-7-8 breathing or progressive muscle relaxation. The staged approach progressively shifts autonomic state.1A cognitive model of insomniaBehaviour Research and Therapy, 40(8), 869–893.2Before-bedtime passive body heating to improve sleepSleep Medicine Reviews, 46, 124–135.
A surgeon adopted a compressed 45-minute version on busy nights. Even abbreviated, her onset dropped from 35 to 12 minutes. The key wasn't perfection — it was any consistent signal chain.
Some wind-down is infinitely better than none. Ideal: 90 minutes. Minimum effective dose: 30 minutes.
16What's the 30-day protocol timeline?
Environmental fixes produce improvement on night one. Circadian alignment stabilises within 5–7 days. Full architecture optimisation takes 3–4 weeks of consistent practice.
Week 1: environmental correction and consistent wake time — fastest returns. Week 2: caffeine timing and wind-down protocol. Week 3: advanced interventions (carb timing, breathing). Week 4: calibration using tracker trends. Biggest subjective shift around days 7–10. Full compounding by day 21–30.1Sleep hygiene in promoting public healthSleep Medicine Reviews, 22, 23–36.2Habit formation in the real worldEJSP, 40(6), 998–1009.
12 startup founders tracked results: Day 3 "onset faster." Day 7 "waking before alarm." Day 14 "afternoon crash gone." Day 30: deep sleep +38%, REM +27%, self-reported energy 2.1→4.2/5.
Quick wins days 1–3, meaningful improvement day 7–10, full transformation day 21–30.
You've explored all 16 questions
Ready to go deeper? The full Sleep Architecture article provides comprehensive frameworks, implementation protocols, and advanced optimization systems.
“The shorter your sleep, the shorter your life.” — Matthew Walker
What You Need to Remember
Why the best performers treat sleep like a non-negotiable skill.
Sleep is engineered 14 hours in advance
Your morning light exposure, 2pm caffeine decision, evening screen habits, and bedroom temperature — decisions spread across the entire day — determine tonight's sleep architecture.
Explore: Module 1 — Sleep Architecture →6.5 hours beats 7 if the timing is right
Sleep cycles in ~90-minute blocks. Waking mid-cycle (at 7 hours) produces worse cognition than completing a cycle at 6 or 7.5 hours. Cycle-aligned waking eliminates morning fog.
Explore: Module 1 — Cycle Timing →10 minutes of morning light changes everything
Bright outdoor light within 30-60 minutes of waking advances your melatonin onset by 1-2 hours and improves sleep latency more reliably than any supplement on the market.
Explore: Module 2 — Light Protocol →Ten days at six hours equals one night of total deprivation
Cumulative sleep restriction produces cognitive impairment indistinguishable from pulling an all-nighter — but the person accumulating the debt can't feel it happening. That's the danger.
Explore: Module 2 — Cumulative Debt →Alcohol destroys the sleep stage you need most
Deep (slow-wave) sleep concentrates growth hormone release, memory consolidation, and immune repair. Alcohol fragments it. Late screens suppress it. Elevated cortisol blocks it. Guard deep sleep.
Explore: Module 3 — Deep Sleep Science →Your 2pm coffee is 25% active at midnight
Caffeine's 5-7 hour half-life means a quarter of that afternoon dose is still blocking adenosine receptors when you're trying to sleep — cutting deep sleep by 15-20% without you noticing.
Explore: Module 3 — Caffeine & Sleep →Drop your core temperature 1-2°F to trigger sleep
A warm bath 90 minutes before bed, a 65-68°F bedroom, and breathable bedding exploit the thermoregulatory sleep trigger — the most underused intervention in sleep optimization.
Explore: Module 4 — Temperature Protocol →You're a poor judge of your own sleep
Subjective sleep ratings overshoot objective quality by 15-30%. People routinely report "great sleep" while wearable data reveals fragmented architecture and minimal deep sleep. Trust the data.
Explore: Module 4 — Sleep Measurement →Same wake time, every day, no exceptions
A fixed wake time (±30 minutes, weekends included) is the single most impactful circadian intervention — more effective than blackout curtains, magnesium, or melatonin combined.
Explore: Module 5 — Consistency Protocol →Treat sleep like a trainable skill
Track, iterate, refine. Sleep responds to deliberate practice the same way any skill does — 4 to 6 weeks of consistent protocol application produces measurable, lasting improvement.
Explore: Module 5 — Building Your Practice →Continue Your Journey
References
0 sources cited — journal articles, foundational texts, and landmark studies in sleep architecture, circadian neuroscience, memory consolidation, and cognitive recovery
- 1(2007). Sleep deprivation: Impact on cognitive performance. Neuropsychiatric Disease and Treatment, 3(5), 553–567.
- 2(2003). The role of actigraphy in the study of sleep and circadian rhythms. Sleep, 26(3), 342–392.
- 3(1990). Subjective and objective sleepiness in the active individual. International Journal of Neuroscience, 52(1-2), 29–37.
- 4(2007). Behavioral and physiological consequences of sleep restriction. Journal of Clinical Sleep Medicine, 3(5), 519–528.
- 5(2013). Sleep deprivation and neurobehavioral dynamics. Current Opinion in Neurobiology, 23(5), 854–863.
- 6(2003). Patterns of performance degradation and restoration during sleep restriction and subsequent recovery. Journal of Sleep Research, 12(1), 1–12.
- 7(2012). Sleep and immune function. Pflügers Archiv-European Journal of Physiology, 463(1), 121–137.
- 8(2009). Adenosine and sleep. Current Neuropharmacology, 7(3), 238–245.
- 9(2010). Hyperarousal and insomnia: State of the science. Sleep Medicine Reviews, 14(1), 9–15.
- 10(1982). A two process model of sleep regulation. Human Neurobiology, 1(3), 195–204.
- 11(2016). The two-process model of sleep regulation: A reappraisal. Journal of Sleep Research, 25(2), 131–143.
- 12(2014). Home lighting before usual bedtime impacts circadian timing. Photochemistry and Photobiology, 90(3), 723–726.
- 13(2014). Sleep health: Can we define it? Does it matter? Sleep, 37(1), 9-17.
- 14(1989). The Pittsburgh Sleep Quality Index: A new instrument. Psychiatry Research, 28(2), 193–213.
- 15(2011). Evening exposure to LED-backlit computer screen affects circadian physiology. Journal of Applied Physiology, 110(5), 1432–1438.
- 16(2005). Normal human sleep: An overview. Principles and Practice of Sleep Medicine, 4, 13–23.
- 17(2015). Evening use of light-emitting eReaders negatively affects sleep. Proceedings of the National Academy of Sciences, 112(4), 1232–1237.
- 18(2009). Duration, timing and quality of sleep are each vital for health, performance and safety. Sleep Health, 1(1), 5–8.
- 19(2010). The memory function of sleep. Nature Reviews Neuroscience, 11(2), 114–126.
- 20(1997). Cumulative sleepiness, mood disturbance, and psychomotor vigilance performance decrements. Sleep, 20(4), 267–277.
- 21(2013). Caffeine effects on sleep taken 0, 3, or 6 hours before going to bed. Journal of Clinical Sleep Medicine, 9(11), 1195–1200.
- 22(2009). Effect of light on human circadian physiology. Sleep Medicine Clinics, 4(2), 165–177.
- 23(2005). Neurocognitive consequences of sleep deprivation. Seminars in Neurology, 25(1), 117–129.
- 24(2013). Alcohol and sleep I: Effects on normal sleep. Alcoholism: Clinical and Experimental Research, 37(4), 539–549.
- 25(2019). Coupled electrophysiological, hemodynamic, and cerebrospinal fluid oscillations in human sleep. Science, 366(6465), 628–631.
- 26(2013). Circadian rhythms, sleep deprivation, and human performance. Progress in Molecular Biology and Translational Science, 119, 155–190.
- 27(2014). The role of sleep in emotional brain function. Annual Review of Clinical Psychology, 10, 679–708.
- 28(2015). Social and behavioral determinants of perceived insufficient sleep. Frontiers in Neurology, 6, 112.
- 29(2002). A cognitive model of insomnia. Behaviour Research and Therapy, 40(8), 869–893.
- 30(1976). A self-assessment questionnaire to determine morningness-eveningness. International Journal of Chronobiology, 4(2), 97–110.
- 31(2012). A paravascular pathway facilitates CSF flow through the brain parenchyma. Science Translational Medicine, 4(147), 147ra111.
- 32(2015). The role of sleep hygiene in promoting public health. Sleep Medicine Reviews, 22, 23–36.
- 33(2010). Effects of sleep deprivation on cognition. Progress in Brain Research, 185, 105–129.
- 34(2015). Sleep, sleep disturbance, and fertility in women. Sleep Medicine Reviews, 22, 78–87.
- 35(2017). The sleep-deprived human brain. Nature Reviews Neuroscience, 18(7), 404–418.
- 36(2010). A meta-analysis of the impact of short-term sleep deprivation on cognitive variables. Psychological Bulletin, 136(3), 375–389.
- 37(2003). High sensitivity of the human circadian melatonin rhythm to resetting by short wavelength light. Journal of Clinical Endocrinology & Metabolism, 88(9), 4502–4505.
- 38(2015). β-amyloid disrupts human NREM slow waves and related memory consolidation. Nature Neuroscience, 18(7), 1051–1057.
- 39(2001). The role of sleep in learning and memory. Science, 294(5544), 1048–1052.
- 40(2007). The contribution of sleep to hippocampus-dependent memory consolidation. Trends in Cognitive Sciences, 11(10), 442–450.
- 41(2013). The critical role of sleep spindles in hippocampal-dependent memory. Journal of Neuroscience, 33(10), 4494–4504.
- 42(2009). Benefits of napping in healthy adults. Journal of Sleep Research, 18(2), 272–281.
- 43(2011). Psychological and behavioral treatments for insomnia I: Approaches and efficacy. In M. H. Kryger, T. Roth, & W. C. Dement (Eds.), Principles and Practice of Sleep Medicine (pp. 866-883). Elsevier. Chapter
- 44(2012). Chronic insomnia. The Lancet, 379(9821), 1129–1141.
- 45(2002). The prefrontal cortex in sleep. Trends in Cognitive Sciences, 6(11), 475–481.
- 46(2010). Dreaming and the brain: From phenomenology to neurophysiology. Trends in Cognitive Sciences, 14(2), 88–100.
- 47(2012). Effects of thermal environment on sleep and circadian rhythm. Journal of Physiological Anthropology, 31(1), 14.
- 48(2008). Short sleep duration and weight gain: A systematic review. Obesity, 16(3), 643–653.
- 49(2013). Sleep homeostasis. Current Opinion in Neurobiology, 23(5), 799–805.
- 50(2013). About sleep's role in memory. Physiological Reviews, 93(2), 681–766.
- 51(2008). Caffeine: Sleep and daytime sleepiness. Sleep Medicine Reviews, 12(2), 153–162.
- 52(2012). Social jetlag and obesity. Current Biology, 22(10), 939–943.
- 53(2005). Hypothalamic regulation of sleep and circadian rhythms. Nature, 437(7063), 1257–1263.
- 54(2015). Sleep, cognition, and normal aging. Perspectives on Psychological Science, 10(1), 97–137.
- 55(2005). Clues to the functions of mammalian sleep. Nature, 437(7063), 1264–1271.
- 56(2016). Effects of diet on sleep quality. Advances in Nutrition, 7(5), 938–949.
- 57(2003). Use of sleep hygiene in the treatment of insomnia. Sleep Medicine Reviews, 7(3), 215–225.
- 58(2005). Sleep-dependent memory consolidation. Nature, 437(7063), 1272–1278.
- 59(2013). Sleep-dependent memory triage. Nature Neuroscience, 16(2), 139–145.
- 60(2014). Sleep and the price of plasticity. Neuron, 81(1), 12–34.
- 61(2008). Metabolic consequences of sleep and sleep loss. Sleep Medicine, 9(Suppl 1), S23–S28.
- 62(2003). The cumulative cost of additional wakefulness. Sleep, 26(2), 117–126.
- 63(2017). Why We Sleep: Unlocking the Power of Sleep and Dreams. Scribner. Book
- 64(2006). Sleep, memory, and plasticity. Annual Review of Psychology, 57, 139–166.
- 65(2007). Jet lag: Trends and coping strategies. The Lancet, 369(9567), 1117–1129.